Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- How To Import Medical Devices Into The USДокумент16 страницHow To Import Medical Devices Into The USliviustitusОценок пока нет
- Referral LetterДокумент2 страницыReferral LetterLyn Escano100% (1)
- Designing and Managing Value Networks and ChannelsДокумент28 страницDesigning and Managing Value Networks and ChannelsLyn EscanoОценок пока нет
- Dri InternshipДокумент38 страницDri InternshipGuruprasad Sanga100% (3)
- PRODUCTION Planning and ControlДокумент14 страницPRODUCTION Planning and ControlLyn EscanoОценок пока нет
- Food and BeverageДокумент35 страницFood and BeverageLyn Escano50% (2)
- Management of Preterm LaborДокумент2 страницыManagement of Preterm LaborpolygoneОценок пока нет
- D6228 - 10Документ8 страницD6228 - 10POSSDОценок пока нет
- HUM110 Gilgamesh EssayДокумент4 страницыHUM110 Gilgamesh EssaynsmeganОценок пока нет
- Health Promotion Officers - CPD Booklet Schedule PDFДокумент5 страницHealth Promotion Officers - CPD Booklet Schedule PDFcharles KadzongaukamaОценок пока нет
- What Is An Abstract of A Thesis ProposalДокумент6 страницWhat Is An Abstract of A Thesis ProposalLyn EscanoОценок пока нет
- Sample Contract of Land SellingДокумент4 страницыSample Contract of Land SellingLyn EscanoОценок пока нет
- Sample Contract of Land SellingДокумент4 страницыSample Contract of Land SellingLyn EscanoОценок пока нет
- Sample Contract of Land SellingДокумент4 страницыSample Contract of Land SellingLyn EscanoОценок пока нет
- PVAO Citizens CharterДокумент26 страницPVAO Citizens CharterLyn EscanoОценок пока нет
- Bite Tight - Angst Fluff Yaoi Exo Ot12 Therewillbe - AsianfanficsДокумент10 страницBite Tight - Angst Fluff Yaoi Exo Ot12 Therewillbe - AsianfanficsLyn EscanoОценок пока нет
- UN OCHA - Oslo Guidelines - The Use of Foreign Military and Civil Defence Assets in Disaster Relief - Nov 2007Документ40 страницUN OCHA - Oslo Guidelines - The Use of Foreign Military and Civil Defence Assets in Disaster Relief - Nov 2007Seni NabouОценок пока нет
- Corporate Social ResponsibilityДокумент3 страницыCorporate Social ResponsibilityLyn EscanoОценок пока нет
- 2014 Training Sked of DOSTДокумент10 страниц2014 Training Sked of DOSTLyn EscanoОценок пока нет
- SPES 2014 Application FormДокумент1 страницаSPES 2014 Application FormCoolbuster.NetОценок пока нет
- Statistics Is The Study of The Collection, Organization, Analysis, Interpretation, andДокумент18 страницStatistics Is The Study of The Collection, Organization, Analysis, Interpretation, andLyn EscanoОценок пока нет
- 12 PIllars of CompetitivenessДокумент12 страниц12 PIllars of CompetitivenessLyn EscanoОценок пока нет
- MaubanДокумент1 страницаMaubanLyn EscanoОценок пока нет
- WarehouseДокумент18 страницWarehouseLyn EscanoОценок пока нет
- ER 2013-01-2012 Yearend ReportДокумент12 страницER 2013-01-2012 Yearend ReportLyn EscanoОценок пока нет
- Chapter 1 - ReportДокумент11 страницChapter 1 - ReportLyn EscanoОценок пока нет
- PART 2 - Chapter 3 Marketing ManagementДокумент42 страницыPART 2 - Chapter 3 Marketing ManagementLyn EscanoОценок пока нет
- Evaluation FormДокумент18 страницEvaluation FormLyn EscanoОценок пока нет
- FEUCAT Form RevisedДокумент2 страницыFEUCAT Form RevisedLyn EscanoОценок пока нет
- Application Water AnalysisДокумент4 страницыApplication Water AnalysisLyn EscanoОценок пока нет
- Basic French Words For TouristsДокумент3 страницыBasic French Words For TouristsLyn EscanoОценок пока нет
- CSForm 100 Rev 2012Документ2 страницыCSForm 100 Rev 2012Agnes Antonio RodriguezОценок пока нет
- Application Form For Accreditation, OSH Practitioner, ConsultantДокумент3 страницыApplication Form For Accreditation, OSH Practitioner, ConsultantLyn EscanoОценок пока нет
- Potato Storage and Processing Potato Storage and Processing: Lighting SolutionДокумент4 страницыPotato Storage and Processing Potato Storage and Processing: Lighting SolutionSinisa SustavОценок пока нет
- Long Term Effects of Surgically Assisted Rapid Maxillary Expansion Without Performing Osteotomy of The Pterygoid PlatesДокумент4 страницыLong Term Effects of Surgically Assisted Rapid Maxillary Expansion Without Performing Osteotomy of The Pterygoid PlatesAngélica Valenzuela AndrighiОценок пока нет
- Aldehydes, Ketones, Carboxylic Acids, and EstersДокумент11 страницAldehydes, Ketones, Carboxylic Acids, and EstersNATURE COMPUTERОценок пока нет
- 204-04B - Tire Pressure Monitoring System (TPMS)Документ23 страницы204-04B - Tire Pressure Monitoring System (TPMS)Sofia AltuzarraОценок пока нет
- Bio411 C1Документ1 страницаBio411 C1Aqiena BalqisОценок пока нет
- Rooftop Rain Water Harvesting in An Educational CampusДокумент9 страницRooftop Rain Water Harvesting in An Educational CampusAkshay BoratiОценок пока нет
- Contractor: Item No. MRS-1st 2021 Ref. Description Unit Quantity Rate of Contractor Unit Rate in Words AmountДокумент1 страницаContractor: Item No. MRS-1st 2021 Ref. Description Unit Quantity Rate of Contractor Unit Rate in Words AmountusmanaliОценок пока нет
- Sample SWMSДокумент4 страницыSample SWMSJuma KavesuОценок пока нет
- Feature: SFP Optical Module 1 .25G Double Optical Fiber 20kmДокумент2 страницыFeature: SFP Optical Module 1 .25G Double Optical Fiber 20kmDaniel Eduardo RodriguezОценок пока нет
- Home Composting SystemsДокумент8 страницHome Composting Systemssumanenthiran123Оценок пока нет
- 'Bubble Kid' Success Puts Gene Therapy Back On TrackДокумент5 страниц'Bubble Kid' Success Puts Gene Therapy Back On TrackAbby Grey Lopez100% (1)
- SPA - MichaelДокумент1 страницаSPA - Michaelgilberthufana446877Оценок пока нет
- IsoTherming® Hydroprocessing TechnologyДокумент4 страницыIsoTherming® Hydroprocessing Technologyromi moriОценок пока нет
- BMJ 40 13Документ8 страницBMJ 40 13Alvin JiwonoОценок пока нет
- User ManualДокумент21 страницаUser ManualKali PrasadОценок пока нет
- BV Lesson Plan 4Документ3 страницыBV Lesson Plan 4api-252119803Оценок пока нет
- Syllabus For Bachelor of Physiotherapy (BPT) Academic ProgrammeДокумент36 страницSyllabus For Bachelor of Physiotherapy (BPT) Academic ProgrammevikasmaeОценок пока нет
- 3 Activities For Adults To Practice Modeling SELДокумент10 страниц3 Activities For Adults To Practice Modeling SELDavid Garcia PerezОценок пока нет
- Scope: Procter and GambleДокумент30 страницScope: Procter and GambleIrshad AhamedОценок пока нет
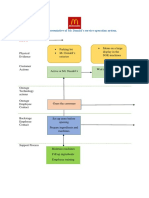
- Blueprint Huynh My Ky Duyen 2022 McDonald'sДокумент2 страницыBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênОценок пока нет
- Review - Practical Accounting 1Документ2 страницыReview - Practical Accounting 1Kath LeynesОценок пока нет
- Narrative Report On Weekly Accomplishments: Department of EducationДокумент2 страницыNarrative Report On Weekly Accomplishments: Department of Educationisha mariano100% (1)
- SanMilan Inigo Cycling Physiology and Physiological TestingДокумент67 страницSanMilan Inigo Cycling Physiology and Physiological Testingjesus.clemente.90Оценок пока нет
- AtelectasisДокумент37 страницAtelectasisSandara ParkОценок пока нет