Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- (FINA1303) (2014) (F) Midterm Yq5j8 42714Документ19 страниц(FINA1303) (2014) (F) Midterm Yq5j8 42714sarah shanОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- As Built - X-Section - 160+700 To 1660+825Документ5 страницAs Built - X-Section - 160+700 To 1660+825Md Mukul MiahОценок пока нет
- Eng 685 Paper 2Документ5 страницEng 685 Paper 2api-531590952Оценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
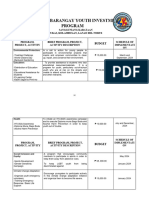
- Annual Barangay Youth Investment ProgramДокумент4 страницыAnnual Barangay Youth Investment ProgramBarangay MukasОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- RA 9072 (National Cave Act)Документ4 страницыRA 9072 (National Cave Act)Lorelain ImperialОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- View of Hebrews Ethan SmithДокумент295 страницView of Hebrews Ethan SmithOlvin Steve Rosales MenjivarОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Case Story: NZS SCM 930 - TransportationДокумент8 страницCase Story: NZS SCM 930 - TransportationJoão Marcelo de CarvalhoОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- 2015.74013.essentials of Spanish With Readings Volume I TextДокумент459 страниц2015.74013.essentials of Spanish With Readings Volume I TextmuytradingsОценок пока нет
- Socialology L1Документ32 страницыSocialology L1Muhammad Waseem YaseenОценок пока нет
- Change Your Life PDF FreeДокумент51 страницаChange Your Life PDF FreeJochebed MukandaОценок пока нет
- Gazette Issued Detailing Functions Under Namal's New MinistryДокумент5 страницGazette Issued Detailing Functions Under Namal's New MinistryDarshana Sanjeewa0% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- People vs. Patulot - Case DigestДокумент5 страницPeople vs. Patulot - Case DigestGendale Am-isОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Deped Order 36Документ22 страницыDeped Order 36Michael Green100% (1)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- UntitledДокумент256 страницUntitledErick RomeroОценок пока нет
- HANA Presented SlidesДокумент102 страницыHANA Presented SlidesRao VedulaОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Michael Ortiz - Loss of Control and Technology Acceptance in (Digital) TransformationДокумент100 страницMichael Ortiz - Loss of Control and Technology Acceptance in (Digital) TransformationMaria Eugenia PuppoОценок пока нет
- Toms River Fair Share Housing AgreementДокумент120 страницToms River Fair Share Housing AgreementRise Up Ocean CountyОценок пока нет
- The Peace Report: Walking Together For Peace (Issue No. 2)Документ26 страницThe Peace Report: Walking Together For Peace (Issue No. 2)Our MoveОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Module 2Документ6 страницModule 2MonicaMartirosyanОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- HBL IPG FAQs PDFДокумент5 страницHBL IPG FAQs PDFAbbas HussainОценок пока нет
- India's Cultural Diplomacy: Present Dynamics, Challenges and Future ProspectsДокумент11 страницIndia's Cultural Diplomacy: Present Dynamics, Challenges and Future ProspectsMAHANTESH GОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Strategy Output Activity (Ppa) : Activities (Ppas) For The Social Sector Activities (Ppas) For The Education Sub-SectorДокумент3 страницыStrategy Output Activity (Ppa) : Activities (Ppas) For The Social Sector Activities (Ppas) For The Education Sub-Sectorstella marizОценок пока нет
- Jose Ferreira Criminal ComplaintДокумент4 страницыJose Ferreira Criminal ComplaintDavid Lohr100% (1)
- Business Forecasting: by ITH PhannyДокумент2 страницыBusiness Forecasting: by ITH PhannysmsОценок пока нет
- IIM Kashipur Master of Business Administration (MBA) Microeconomics, Term I, Academic Year 2021-2022 Syllabus I. Instructor DetailДокумент20 страницIIM Kashipur Master of Business Administration (MBA) Microeconomics, Term I, Academic Year 2021-2022 Syllabus I. Instructor DetailSai Teja MekalaОценок пока нет
- Principles of ManagementДокумент107 страницPrinciples of ManagementalchemistОценок пока нет
- Wa0256.Документ3 страницыWa0256.Daniela Daza HernándezОценок пока нет
- Dayalbagh HeraldДокумент7 страницDayalbagh HeraldRavi Kiran MaddaliОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- 9th SemДокумент90 страниц9th SemVamsi MajjiОценок пока нет
- Rule: Airworthiness Directives: Hartzell Propeller Inc.Документ3 страницыRule: Airworthiness Directives: Hartzell Propeller Inc.Justia.comОценок пока нет