Вам также может понравиться
- 404 RДокумент1 страница404 Rapi-253598260Оценок пока нет
- Administrator (Administrator#)Документ26 страницAdministrator (Administrator#)api-253598260Оценок пока нет
- 409 PДокумент9 страниц409 Papi-253598260Оценок пока нет
- 409 RДокумент1 страница409 Rapi-253598260Оценок пока нет
- 317 RДокумент1 страница317 Rapi-253598260Оценок пока нет
- 405 RДокумент1 страница405 Rapi-253598260Оценок пока нет
- Administrator (Administrator#)Документ26 страницAdministrator (Administrator#)api-253598260Оценок пока нет
- 317 RДокумент1 страница317 Rapi-253598260Оценок пока нет
- 406 PДокумент39 страниц406 Papi-253598260Оценок пока нет
- 406 RДокумент1 страница406 Rapi-253598260Оценок пока нет
- 404 PДокумент25 страниц404 Papi-253598260Оценок пока нет
- 403 PДокумент5 страниц403 Papi-253598260Оценок пока нет
- 403 RДокумент1 страница403 Rapi-253598260Оценок пока нет
- 481 PДокумент12 страниц481 Papi-253598260Оценок пока нет
- 407 RДокумент1 страница407 Rapi-253598260Оценок пока нет
- 1 Part 2 Final: Cloud-Based GIS Maps Displaying Aggregate Data On Medical MalpracticeДокумент11 страниц1 Part 2 Final: Cloud-Based GIS Maps Displaying Aggregate Data On Medical Malpracticeapi-253598260Оценок пока нет
- 481 RДокумент1 страница481 Rapi-253598260Оценок пока нет
- 408 PДокумент36 страниц408 Papi-253598260Оценок пока нет
- 408 RДокумент1 страница408 Rapi-253598260Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Documentation Sheet Sterilization EnglishДокумент2 страницыDocumentation Sheet Sterilization EnglishBanita CarmenОценок пока нет
- Giant Cell Tumor of Bone - An Overview: Current Concepts ReviewДокумент8 страницGiant Cell Tumor of Bone - An Overview: Current Concepts ReviewDwi fitria nivaОценок пока нет
- Product PlanДокумент19 страницProduct Planlily30109150% (2)
- Safety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingДокумент11 страницSafety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingShahid BhattiОценок пока нет
- Role of Hospital Pharmacist in Handling Radio Active SubstanceДокумент5 страницRole of Hospital Pharmacist in Handling Radio Active SubstanceAashish BhattaraiОценок пока нет
- Taylan Competency NeedsДокумент32 страницыTaylan Competency NeedsLovejoice Cha NnelОценок пока нет
- Adver PaperДокумент10 страницAdver PaperDee Jay de JesusОценок пока нет
- PДокумент3 страницыPPamela GuevaraОценок пока нет
- MoH - Uganda RBF Program Hospital Quartely Quality Assessment Tool - Jan 2019Документ31 страницаMoH - Uganda RBF Program Hospital Quartely Quality Assessment Tool - Jan 2019Steven SsemwangaОценок пока нет
- 2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST Segment ElevationДокумент66 страниц2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST Segment ElevationMoises Torres AlvarezОценок пока нет
- Risk Management Plan TemplateДокумент10 страницRisk Management Plan Templateamit singh0% (1)
- Pathologist Job SpecificationДокумент16 страницPathologist Job SpecificationLalaluluОценок пока нет
- Aspiracion Destornillador Implanto Roa-V1-Id1018Документ3 страницыAspiracion Destornillador Implanto Roa-V1-Id1018CesarAmorotoОценок пока нет
- Human Rights (ROTC)Документ6 страницHuman Rights (ROTC)shujin_samaОценок пока нет
- Nursepreneurs Essay by J. BacarisasДокумент17 страницNursepreneurs Essay by J. BacarisasCris GalendezОценок пока нет
- Applying A Feminist Lens To Indias Foreign Policy A Compendium of EssaysДокумент124 страницыApplying A Feminist Lens To Indias Foreign Policy A Compendium of EssaysRasced AliОценок пока нет
- Blue Green Yellow Modern English Intrapersonal Communication Educational Presentation - 20231109 - FixДокумент12 страницBlue Green Yellow Modern English Intrapersonal Communication Educational Presentation - 20231109 - FixmhailvandalzОценок пока нет
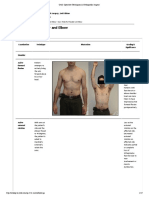
- Exam Table For Shoulder and ElbowДокумент17 страницExam Table For Shoulder and ElbowLouie OkayОценок пока нет
- BAYBAY AwardsДокумент63 страницыBAYBAY AwardsClennil Palmes SustraidoОценок пока нет
- 2021 A Guide To The African Human Rights System Celebrating 40 YearsДокумент115 страниц2021 A Guide To The African Human Rights System Celebrating 40 YearsChala Yuye KemerОценок пока нет
- Ejsr Vol 97 Issue 1 159 171Документ171 страницаEjsr Vol 97 Issue 1 159 171Raja ChandruОценок пока нет
- Antimicrobial Products-Test For Antimicrobial Activity and EfficacyДокумент14 страницAntimicrobial Products-Test For Antimicrobial Activity and EfficacyherfuentesОценок пока нет
- POCSOДокумент15 страницPOCSOThakur Avnish Singh100% (1)
- Internet Addiction - ResearchДокумент13 страницInternet Addiction - ResearchpipedsОценок пока нет
- Genesis Platinum Manual 8090Документ23 страницыGenesis Platinum Manual 8090Huni BuniОценок пока нет
- UConn Prosthodontics Clinic Manual 12-13Документ69 страницUConn Prosthodontics Clinic Manual 12-13lippincott2011Оценок пока нет
- Vulture ConservationДокумент14 страницVulture ConservationSaba Parvin Haque100% (2)
- Review Jurnal Varicella - Dewi Manik Aulia Fadli - 16700096Документ26 страницReview Jurnal Varicella - Dewi Manik Aulia Fadli - 16700096Lia FadliОценок пока нет
- Understanding and Completing The Reversion (25pp)Документ25 страницUnderstanding and Completing The Reversion (25pp)Tony Lambert100% (3)
- Minimall Tooth Preparation Garil GurelДокумент13 страницMinimall Tooth Preparation Garil GurelMónica BecerraОценок пока нет