Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- SUMAN Guideline 2020 Web VersionДокумент84 страницыSUMAN Guideline 2020 Web VersionJasoners22333Оценок пока нет
- Pregnancy: Postpartum and Newborn Referral Services 1Документ6 страницPregnancy: Postpartum and Newborn Referral Services 1aufcheОценок пока нет
- Obs MCQДокумент13 страницObs MCQaaycee100% (3)
- Preterm Birth - Risk Factors, Interventions For Risk Reduction, and Maternal Prognosis - UpToDateДокумент55 страницPreterm Birth - Risk Factors, Interventions For Risk Reduction, and Maternal Prognosis - UpToDateArnold Yesid Rivas ZapataОценок пока нет
- Sagum, Diana Rose - (Pelvic)Документ1 страницаSagum, Diana Rose - (Pelvic)AUSTRIAN DIAGNOSTIC CENTERОценок пока нет
- Quiz On PGD (M103)Документ25 страницQuiz On PGD (M103)Mickael Josef TabrillaОценок пока нет
- Multi Fetal Pregnancy & ComplicationsДокумент20 страницMulti Fetal Pregnancy & Complicationsapi-3705046Оценок пока нет
- Tantangan Kesehatan Mental Pada Periode Hamil, NifasДокумент112 страницTantangan Kesehatan Mental Pada Periode Hamil, NifasAdefitriaОценок пока нет
- Serdang Protocol ObgynДокумент152 страницыSerdang Protocol ObgynNadhirah ZulkifliОценок пока нет
- Preboard RMДокумент3 страницыPreboard RMJonas Marvin Anaque0% (1)
- Monitoring Uterine ContractionsДокумент23 страницыMonitoring Uterine ContractionsCristin UngabОценок пока нет
- Biophysical ProfileДокумент8 страницBiophysical ProfileAmritaОценок пока нет
- UntitledДокумент10 страницUntitledMitsury Jacqueline Flores C.Оценок пока нет
- Journal 1Документ4 страницыJournal 1Kristoff CamposОценок пока нет
- Efektifitas Pemberian Wedang Jahe Terhadap Frekuensi Mual Dan Muntah Pada Ibu Hamil Trimester I Di Kabupaten Bengkulu Utara TAHUN 2017Документ11 страницEfektifitas Pemberian Wedang Jahe Terhadap Frekuensi Mual Dan Muntah Pada Ibu Hamil Trimester I Di Kabupaten Bengkulu Utara TAHUN 2017rohyatiОценок пока нет
- KTI Bahasa InggrisДокумент6 страницKTI Bahasa InggrisNurHana RamadhanОценок пока нет
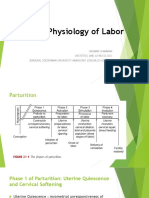
- Physiology of LaborДокумент17 страницPhysiology of Laborsennaavia12Оценок пока нет
- Hipertensi Pada Ibu Hamil Trimester 3Документ8 страницHipertensi Pada Ibu Hamil Trimester 3deskha putriОценок пока нет
- Management During Labor of Multiple Pregnancy: Manish Gupta Roll No-47Документ10 страницManagement During Labor of Multiple Pregnancy: Manish Gupta Roll No-47manishОценок пока нет
- Fetal Mummification in CowsДокумент22 страницыFetal Mummification in CowsTahseen AlamОценок пока нет
- Trial of ScarДокумент12 страницTrial of Scarnyangara50% (2)
- Corrigendum: Sun Kyung Kim, Seyeon Park, Jiwon Oh, Jisoon Kim, Sukhee AhnДокумент6 страницCorrigendum: Sun Kyung Kim, Seyeon Park, Jiwon Oh, Jisoon Kim, Sukhee AhnEmmanuel MpaliyeОценок пока нет
- Multiple Pregnancy - PPTX Md3Документ41 страницаMultiple Pregnancy - PPTX Md3Brother George100% (1)
- A Position Paper On The Illegalization of Abortion in The PhilippinesДокумент3 страницыA Position Paper On The Illegalization of Abortion in The PhilippinesCristine Joy Remerata Villarosa80% (148)
- Case Reports in Women's Health: Tanja Baltus Maria Luisa MartinДокумент2 страницыCase Reports in Women's Health: Tanja Baltus Maria Luisa MartinDavid LacosteОценок пока нет
- Antepartum 1Документ3 страницыAntepartum 1Emily DavisОценок пока нет
- Introduction of Labour MonitoringДокумент29 страницIntroduction of Labour MonitoringMishti MokarramaОценок пока нет
- BJOG - 2023 - Category Abortion CareДокумент3 страницыBJOG - 2023 - Category Abortion Care75dcqkm4nwОценок пока нет
- Breech DeliveryДокумент73 страницыBreech DeliveryFebriendo Vanni Dwi JayantiОценок пока нет
- CC Chua, Prince Robert C. Reflection Paper 4AДокумент1 страницаCC Chua, Prince Robert C. Reflection Paper 4APrince Robert ChuaОценок пока нет