Вам также может понравиться
- The Biopsychosocial ModelДокумент8 страницThe Biopsychosocial ModelOlaya HernándezОценок пока нет
- Study Guide to Accompany Physiological Psychology Brown/WallaceОт EverandStudy Guide to Accompany Physiological Psychology Brown/WallaceОценок пока нет
- Psychiatric Diagnosis: Challenges and ProspectsОт EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumРейтинг: 5 из 5 звезд5/5 (1)
- Racism and Psychiatry: Contemporary Issues and InterventionsОт EverandRacism and Psychiatry: Contemporary Issues and InterventionsMorgan M. MedlockОценок пока нет
- Somatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesОт EverandSomatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesChristos CharisОценок пока нет
- Current Topics in Clinical and Community Psychology: Volume 3От EverandCurrent Topics in Clinical and Community Psychology: Volume 3Рейтинг: 3 из 5 звезд3/5 (1)
- Comprehensive Handbook of Clinical Health PsychologyОт EverandComprehensive Handbook of Clinical Health PsychologyBret A BoyerОценок пока нет
- Advances in Cognitive—Behavioral Research and Therapy: Volume 5От EverandAdvances in Cognitive—Behavioral Research and Therapy: Volume 5Оценок пока нет
- Ethical Issues in Clinical Forensic PsychiatryОт EverandEthical Issues in Clinical Forensic PsychiatryArtemis IgoumenouОценок пока нет
- Amnesia: Clinical, Psychological and Medicolegal AspectsОт EverandAmnesia: Clinical, Psychological and Medicolegal AspectsC. W. M. WhittyОценок пока нет
- Medical Psychology: Contributions to Behavioral MedicineОт EverandMedical Psychology: Contributions to Behavioral MedicineCharles K. ProkopОценок пока нет
- Without Stigma: About the Stigma and the Identity of the Mental IllnessОт EverandWithout Stigma: About the Stigma and the Identity of the Mental IllnessОценок пока нет
- The Essential Practitioner's Handbook of Personal Construct PsychologyОт EverandThe Essential Practitioner's Handbook of Personal Construct PsychologyОценок пока нет
- Development of Perception: Psychobiological PerspectivesОт EverandDevelopment of Perception: Psychobiological PerspectivesRichard AslinОценок пока нет
- Staying Well After Psychosis: A Cognitive Interpersonal Approach to Recovery and Relapse PreventionОт EverandStaying Well After Psychosis: A Cognitive Interpersonal Approach to Recovery and Relapse PreventionОценок пока нет
- Annual Review of Addictions and Offender Counseling II: Best PracticesОт EverandAnnual Review of Addictions and Offender Counseling II: Best PracticesОценок пока нет
- Family Violence: Explanations and Evidence-Based Clinical PracticeОт EverandFamily Violence: Explanations and Evidence-Based Clinical PracticeОценок пока нет
- Emotional Competence: The Fountain of personal, professional and private SuccessОт EverandEmotional Competence: The Fountain of personal, professional and private SuccessОценок пока нет
- Handbook of Forensic Assessment: Psychological and Psychiatric PerspectivesОт EverandHandbook of Forensic Assessment: Psychological and Psychiatric PerspectivesРейтинг: 4 из 5 звезд4/5 (1)
- The Wiley-Blackwell Handbook of Addiction PsychopharmacologyОт EverandThe Wiley-Blackwell Handbook of Addiction PsychopharmacologyОценок пока нет
- The Trauma of Sexual Assault: Treatment, Prevention and PracticeОт EverandThe Trauma of Sexual Assault: Treatment, Prevention and PracticeJenny PetrakРейтинг: 5 из 5 звезд5/5 (1)
- Depression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesОт EverandDepression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesChristos CharisОценок пока нет
- Treatment and Prevention of Alcohol Problems: A Resource ManualОт EverandTreatment and Prevention of Alcohol Problems: A Resource ManualОценок пока нет
- Sexual Assault Risk Reduction and Resistance: Theory, Research, and PracticeОт EverandSexual Assault Risk Reduction and Resistance: Theory, Research, and PracticeLindsay M. OrchowskiОценок пока нет
- Guilt and ChildrenОт EverandGuilt and ChildrenJane BybeeОценок пока нет
- Cognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationОт EverandCognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationMark MuseОценок пока нет
- Psychotherapy Pearls: Critical Insights for Doing PsychotherapyОт EverandPsychotherapy Pearls: Critical Insights for Doing PsychotherapyОценок пока нет
- Origins of Phobias and Anxiety Disorders: Why More Women than Men?От EverandOrigins of Phobias and Anxiety Disorders: Why More Women than Men?Оценок пока нет
- Medical Intimacy: Deeper Understanding Allows for Deeper HealingОт EverandMedical Intimacy: Deeper Understanding Allows for Deeper HealingОценок пока нет
- The Wiley Handbook on Offenders with Intellectual and Developmental Disabilities: Research, Training, and PracticeОт EverandThe Wiley Handbook on Offenders with Intellectual and Developmental Disabilities: Research, Training, and PracticeОценок пока нет
- Preventing Dementia?: Critical Perspectives on a New Paradigm of Preparing for Old AgeОт EverandPreventing Dementia?: Critical Perspectives on a New Paradigm of Preparing for Old AgeОценок пока нет
- Progress in Neurology and Psychiatry: An Annual ReviewОт EverandProgress in Neurology and Psychiatry: An Annual ReviewE. A. SpiegelОценок пока нет
- Solution Focused Harm Reduction: Working effectively with people who misuse substancesОт EverandSolution Focused Harm Reduction: Working effectively with people who misuse substancesОценок пока нет
- Psychological Trauma and Ptsd/Soldiers (Child)От EverandPsychological Trauma and Ptsd/Soldiers (Child)Оценок пока нет
- Medical Conditions Associated with Suicide Risk: Amputation and SuicideОт EverandMedical Conditions Associated with Suicide Risk: Amputation and SuicideОценок пока нет
- Changing Trends in Mental Health Care and Research in GhanaОт EverandChanging Trends in Mental Health Care and Research in GhanaОценок пока нет
- Summary of The Plot to Destroy Trump: How the Deep State Fabricated the Russian Dossier to Subvert the PresidentОт EverandSummary of The Plot to Destroy Trump: How the Deep State Fabricated the Russian Dossier to Subvert the PresidentОценок пока нет
- Hallucination, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHallucination, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- A Guide for Treating Adolescent Sexual Abusers in Residential Settings: Forty-Five Days at a Time: a Collaborative EffortОт EverandA Guide for Treating Adolescent Sexual Abusers in Residential Settings: Forty-Five Days at a Time: a Collaborative EffortОценок пока нет
- Psychiatric Emergencies and the Law: The Impact of the Mental Health Act (1959)От EverandPsychiatric Emergencies and the Law: The Impact of the Mental Health Act (1959)Оценок пока нет
- Beg Swimming TechniqueДокумент17 страницBeg Swimming Techniquevirpara100% (1)
- A Rooms (1603-1856) B Rooms (1903-2156) C Rooms (2203-2456) D Rooms (2503-2756) E Rooms (2803-3056)Документ1 страницаA Rooms (1603-1856) B Rooms (1903-2156) C Rooms (2203-2456) D Rooms (2503-2756) E Rooms (2803-3056)Billy CooperОценок пока нет
- Sy Rules 20132017Документ70 страницSy Rules 20132017Billy CooperОценок пока нет
- CT MMB 073Документ2 страницыCT MMB 073Billy CooperОценок пока нет
- 1 s2.0 S0272735813001566 MainДокумент19 страниц1 s2.0 S0272735813001566 MainBilly CooperОценок пока нет
- NHS Choices - Delivering For The NHSДокумент24 страницыNHS Choices - Delivering For The NHSJames BarracloughОценок пока нет
- The Habitus Process A Biopsychosocial Conception: Andreas PickelДокумент36 страницThe Habitus Process A Biopsychosocial Conception: Andreas PickelBilly CooperОценок пока нет
- 1 s2.0 S0272494409000486 MainДокумент12 страниц1 s2.0 S0272494409000486 MainBilly CooperОценок пока нет
- Tips For Writing A Critical EssayДокумент2 страницыTips For Writing A Critical EssayBilly CooperОценок пока нет
- The Habitus Process A Biopsychosocial Conception: Andreas PickelДокумент36 страницThe Habitus Process A Biopsychosocial Conception: Andreas PickelBilly CooperОценок пока нет
- Psychometric Perspectives On Diagnostic Systems: Denny BorsboomДокумент20 страницPsychometric Perspectives On Diagnostic Systems: Denny BorsboomBilly CooperОценок пока нет
- Clinical Psychology: Five Classes of Research Questions in Clinical PsychologyДокумент12 страницClinical Psychology: Five Classes of Research Questions in Clinical PsychologycarlammartinsОценок пока нет
- 1 s2.0 S0272735813001566 MainДокумент19 страниц1 s2.0 S0272735813001566 MainBilly CooperОценок пока нет
- Batson & Ahmad (In Press)Документ65 страницBatson & Ahmad (In Press)Billy CooperОценок пока нет
- 1 s2.0 S0167487011001589 MainДокумент11 страниц1 s2.0 S0167487011001589 MainBilly CooperОценок пока нет
- Cohen 2007 Stress and DiseaseДокумент3 страницыCohen 2007 Stress and DiseaseBilly CooperОценок пока нет
- Eco Anthro 22Документ110 страницEco Anthro 22Billy CooperОценок пока нет
- Essaywriting 131213020540 Phpapp01Документ5 страницEssaywriting 131213020540 Phpapp01api-235870670Оценок пока нет
- Chandola 2008 Unhealthy Behaviours Stress and CHDДокумент9 страницChandola 2008 Unhealthy Behaviours Stress and CHDBilly CooperОценок пока нет
- Psychological Approach To Successful Ageing Predicts Future Quality of Life in Older AdultsДокумент10 страницPsychological Approach To Successful Ageing Predicts Future Quality of Life in Older AdultsBilly CooperОценок пока нет
- Positive Psychologists On Positive Psychology: Ilona BoniwellДокумент6 страницPositive Psychologists On Positive Psychology: Ilona BoniwellBilly Cooper100% (1)
- Chronic Illness 2011 Michalak 209 24Документ17 страницChronic Illness 2011 Michalak 209 24Billy CooperОценок пока нет
- Positive Psychologists On Positive Psychology: Ilona BoniwellДокумент6 страницPositive Psychologists On Positive Psychology: Ilona BoniwellBilly Cooper100% (1)
- 10 Minute Trainer Accelerated Schedule1Документ1 страница10 Minute Trainer Accelerated Schedule1Billy CooperОценок пока нет
- Mac BrushДокумент1 страницаMac BrushBilly CooperОценок пока нет
- Psychology and Aging: PsychologistsДокумент8 страницPsychology and Aging: PsychologistsThamer SamhaОценок пока нет
- 1 s2.0 S0005796711000234 MainДокумент8 страниц1 s2.0 S0005796711000234 MainBilly CooperОценок пока нет
- Lab 5: Digital Phase Locked Loop (PLL) : Matlab Part: ObjectiveДокумент11 страницLab 5: Digital Phase Locked Loop (PLL) : Matlab Part: ObjectiveThế Anh NguyễnОценок пока нет
- ME2142-2 Lab MAnual Speed and Position ControlДокумент9 страницME2142-2 Lab MAnual Speed and Position ControlMohammad Taha IrfanОценок пока нет
- Ornek SorularДокумент27 страницOrnek SorularFatih ErogluОценок пока нет
- Automation Expo Exhibitior List 2015Документ92 страницыAutomation Expo Exhibitior List 2015Manan TyagiОценок пока нет
- The Raise of Robots and AiДокумент11 страницThe Raise of Robots and AiyazhinijainvidhyalaОценок пока нет
- 2.37 Tuning Interacting Loops, Synchronizing Loops: M. RuelДокумент4 страницы2.37 Tuning Interacting Loops, Synchronizing Loops: M. RuelSergioОценок пока нет
- MCS 014Документ2 страницыMCS 014jammu_rachnaОценок пока нет
- CS2301-Software Engineering 2 MarksДокумент17 страницCS2301-Software Engineering 2 MarksDhanusha Chandrasegar SabarinathОценок пока нет
- Metallurgical Thermo DynamicsДокумент567 страницMetallurgical Thermo Dynamicspahnin100% (4)
- Process Instrumentation 2Документ8 страницProcess Instrumentation 2Aditya RasalОценок пока нет
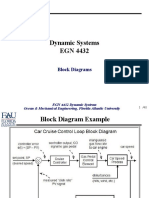
- Dynamic Systems EGN 4432: Block DiagramsДокумент40 страницDynamic Systems EGN 4432: Block DiagramsKeyvon AndersonОценок пока нет
- Manul of Multi-Frequency Remote Control Duplicator (New)Документ11 страницManul of Multi-Frequency Remote Control Duplicator (New)Eduardo RoqueОценок пока нет
- DZone ScyllaDB Database Systems Trend ReportДокумент49 страницDZone ScyllaDB Database Systems Trend ReportSidharth PallaiОценок пока нет
- 158LAB2Документ6 страниц158LAB2Asghar JafariОценок пока нет
- 3 - Optimization ModelsДокумент13 страниц3 - Optimization ModelsMuhammad EzzatОценок пока нет
- Research Paper PresentationДокумент23 страницыResearch Paper PresentationVasishthОценок пока нет
- Dense NetДокумент28 страницDense NetFahad RazaОценок пока нет
- Trade-Off Examples Inside Software Engineering and Computer ScienceДокумент6 страницTrade-Off Examples Inside Software Engineering and Computer SciencePradip PawarОценок пока нет
- OEE ExplainedДокумент3 страницыOEE Explainedvvv5452100% (2)
- Chapter 07 Entropy-7 PDFДокумент35 страницChapter 07 Entropy-7 PDFMarviandi EkoОценок пока нет
- Lecture 1Документ13 страницLecture 1Syed Hussain Akbar MosviОценок пока нет
- Introduction To Mechatronics SystemДокумент8 страницIntroduction To Mechatronics SystemSomalia WadankeygaОценок пока нет
- 3-2-9 - Soft Computing LabДокумент2 страницы3-2-9 - Soft Computing LabarunkumargogeОценок пока нет
- Machine Learning For Complex and Unmanned Systems: February 2024Документ2 страницыMachine Learning For Complex and Unmanned Systems: February 2024Dương Trần Mỹ LinhОценок пока нет
- A Simulation-Enhanced Lean Design Process PDFДокумент24 страницыA Simulation-Enhanced Lean Design Process PDFAngela CastilloОценок пока нет
- Chapter 10Документ8 страницChapter 10Aldon JimenezОценок пока нет
- Load Positioning and Minimization of Load Oscillations in Rotary CranesДокумент13 страницLoad Positioning and Minimization of Load Oscillations in Rotary CranesAnonymous LFgO4WbIDОценок пока нет
- Testing PrimerДокумент43 страницыTesting PrimerAndrei CiobanuОценок пока нет
- Obstacle Avoidance Based On Fuzzy LogicДокумент5 страницObstacle Avoidance Based On Fuzzy LogicMarcAlomarPayerasОценок пока нет
- Decision Support System & Management Information SystemДокумент3 страницыDecision Support System & Management Information SystemJacob Snyder100% (1)