Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- A Brief List of Old Wives TalesДокумент3 страницыA Brief List of Old Wives TalesMelissaОценок пока нет
- About VaginaДокумент13 страницAbout VaginaRazend Muhd0% (1)
- Toolbox Talk CylindersДокумент1 страницаToolbox Talk CylindersAdel SukerОценок пока нет
- Toolbox Talk CylindersДокумент1 страницаToolbox Talk CylindersAdel SukerОценок пока нет
- قواعد الانجليزية كاملة اهداء صفحة المدرس بوكДокумент40 страницقواعد الانجليزية كاملة اهداء صفحة المدرس بوكboudekhanaОценок пока нет
- Toolbox Talk ConstructionДокумент1 страницаToolbox Talk ConstructionAdel Suker100% (1)
- Toolbox Talk ErgonomicsДокумент1 страницаToolbox Talk ErgonomicsAdel SukerОценок пока нет
- Toolbox Talk Fire SafetyДокумент1 страницаToolbox Talk Fire SafetyAdel Suker0% (1)
- Bott Mech Toolbox TalksДокумент266 страницBott Mech Toolbox TalksAdel SukerОценок пока нет
- F. Y. B. Sc. (Zoology) Question BankДокумент51 страницаF. Y. B. Sc. (Zoology) Question BankHassan Ahmed100% (2)
- Incident Report of BP TexasДокумент341 страницаIncident Report of BP TexasUmar Khan100% (1)
- Case Presentation PreeclampsiaДокумент41 страницаCase Presentation PreeclampsiaJomari Zapanta50% (2)
- Toolbox Talk DrivingДокумент1 страницаToolbox Talk DrivingAdel SukerОценок пока нет
- Toolbox Talk DrivingДокумент1 страницаToolbox Talk DrivingAdel SukerОценок пока нет
- Toolbox Talk ElectricalДокумент1 страницаToolbox Talk ElectricalAdel Suker100% (1)
- Classification of Neutrophilic Granulocytes 2000Документ1 страницаClassification of Neutrophilic Granulocytes 2000Gregorio De Las Casas100% (1)
- Oil and Gas Revision 2Документ11 страницOil and Gas Revision 2Adel SukerОценок пока нет
- National Geographic Little Kids - 03 2019 - 04 2019Документ35 страницNational Geographic Little Kids - 03 2019 - 04 2019florenciaОценок пока нет
- Unit 3 Admission Procedure of Women in LabourДокумент30 страницUnit 3 Admission Procedure of Women in LabourNishaThakuriОценок пока нет
- ImpressionДокумент7 страницImpressionAnnisa Nur AmalaОценок пока нет
- GRI 2: General Disclosures 2021: Universal StandardДокумент58 страницGRI 2: General Disclosures 2021: Universal StandardAlfita PutrimasiОценок пока нет
- Vacuum Leak Test ProcedureДокумент6 страницVacuum Leak Test ProcedureTomy George100% (4)
- Modelconfspace PDFДокумент13 страницModelconfspace PDFAdel SukerОценок пока нет
- TENSESДокумент9 страницTENSESworld of innovationОценок пока нет
- Tenses TableДокумент5 страницTenses Tableapi-314670535Оценок пока нет
- Indg402 PDFДокумент7 страницIndg402 PDFKheireddine AounallahОценок пока нет
- Location of West, Texas, Plant ExplosionДокумент1 страницаLocation of West, Texas, Plant ExplosionThe State Newspaper0% (1)
- IOC Fire IncidentДокумент32 страницыIOC Fire Incidentnimesh_patel_indira101Оценок пока нет
- ASCO Final v1 ColorДокумент10 страницASCO Final v1 ColorAdel SukerОценок пока нет
- Toolbox Talk BiospillДокумент1 страницаToolbox Talk BiospillAdel SukerОценок пока нет
- Toolbox Talk ConfspaceДокумент1 страницаToolbox Talk ConfspaceAdel SukerОценок пока нет
- Toolbox Talk BiospillДокумент1 страницаToolbox Talk BiospillAdel SukerОценок пока нет
- tbt3 TДокумент1 страницаtbt3 TAdel SukerОценок пока нет
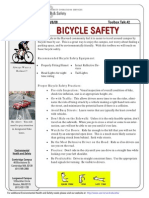
- Toolbox Talk BicycleДокумент1 страницаToolbox Talk BicycleAdel SukerОценок пока нет
- Conabeare Acoustics Tool Box Talks July 2010Документ126 страницConabeare Acoustics Tool Box Talks July 2010Adel SukerОценок пока нет
- NZ Fire Behaviour Toolkit: User Guide and Technical: June 2008Документ32 страницыNZ Fire Behaviour Toolkit: User Guide and Technical: June 2008Adel SukerОценок пока нет
- Special Edition Fire BehaviorДокумент11 страницSpecial Edition Fire BehaviorAdel SukerОценок пока нет
- HK Ocean Park (Wednesday 8am) (Read-Only)Документ22 страницыHK Ocean Park (Wednesday 8am) (Read-Only)Ajay GopalОценок пока нет
- 2.movers Pratice Test - RW Part 1 - 2Документ20 страниц2.movers Pratice Test - RW Part 1 - 2Ngoc Huyen HoangОценок пока нет
- Ang Inahing Manok at Ang Kanyang Mga SisiwДокумент13 страницAng Inahing Manok at Ang Kanyang Mga SisiwKaren Kichelle Navarro EviaОценок пока нет
- The Revision Test 2014Документ3 страницыThe Revision Test 2014Danang SatrioОценок пока нет
- UntitledДокумент41 страницаUntitledReham Ricka ValmonteОценок пока нет
- Articles, Determiners & Quantifiers Set 1Документ25 страницArticles, Determiners & Quantifiers Set 1fatoОценок пока нет
- Activity Book 1º - EstudianteДокумент89 страницActivity Book 1º - EstudianteJULIO CESARОценок пока нет
- Budidaya Maggot Lalat Black Soldier Flies (BSF) Sebagai Pakan TernakДокумент5 страницBudidaya Maggot Lalat Black Soldier Flies (BSF) Sebagai Pakan TernakMiqdadОценок пока нет
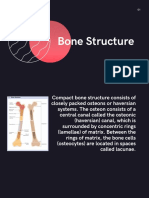
- Topic PPT Bone StructureДокумент14 страницTopic PPT Bone StructureMoonОценок пока нет
- Exam (1) On Unit (1) :: Connect Plus 4 - 1st TermДокумент12 страницExam (1) On Unit (1) :: Connect Plus 4 - 1st TermHassan k1455 rashidОценок пока нет
- Mixed Dentition AnalysisДокумент6 страницMixed Dentition AnalysisJess JesiОценок пока нет
- Learn English Podcasts Elementary 01 02 TranscriptДокумент5 страницLearn English Podcasts Elementary 01 02 TranscriptrosebudkstОценок пока нет
- Types of Reproduction: Sexual AsexualДокумент45 страницTypes of Reproduction: Sexual AsexualasdОценок пока нет
- Chapter-2 Profile of Karbi Anglong DistrictДокумент37 страницChapter-2 Profile of Karbi Anglong DistrictDiganta Kumar GogoiОценок пока нет
- Animals SimilesДокумент1 страницаAnimals SimilesacademiaedelОценок пока нет
- a hero of our time (当代英雄)Документ165 страницa hero of our time (当代英雄)JingОценок пока нет
- Hydrocoele PDFДокумент1 страницаHydrocoele PDFSaugat PantОценок пока нет
- The Warm-Up: Sabina Rubio SánchezДокумент19 страницThe Warm-Up: Sabina Rubio Sánchezsabirubiosa5741Оценок пока нет
- TESTДокумент5 страницTESTnoralizaaliОценок пока нет
- L4 Directed Writing Insert ZooparkДокумент4 страницыL4 Directed Writing Insert ZooparkPranavОценок пока нет
- Family Members Possessive CaseДокумент6 страницFamily Members Possessive CaseClaudia SamfiraОценок пока нет
- Clavus, Ingrown Nail, Skin Epithelial CystsДокумент11 страницClavus, Ingrown Nail, Skin Epithelial CystsRafiОценок пока нет