Вам также может понравиться
- ANSI Emergency Eyewash StandardДокумент28 страницANSI Emergency Eyewash StandardWilliam Condori Rafael100% (3)
- IsO PAS223 Provides International Best PracticeДокумент5 страницIsO PAS223 Provides International Best PracticeAntónio FerreiraОценок пока нет
- (III) PSSR PROCEDURE (Rev00) PDFДокумент17 страниц(III) PSSR PROCEDURE (Rev00) PDFDen Bagus Blitar100% (5)
- Fraser2016 PDFДокумент10 страницFraser2016 PDFNoviansyah PamungkasОценок пока нет
- Change Management: Ford Motor CompanyДокумент9 страницChange Management: Ford Motor CompanyDarien Tayag Aloro0% (1)
- CASH Report 10 - 2012 FINAL PDF Nettiin1Документ118 страницCASH Report 10 - 2012 FINAL PDF Nettiin1sabahaizatОценок пока нет
- EMCO Induction and Training ProcedureДокумент11 страницEMCO Induction and Training ProcedureAnonymous ocCa18RОценок пока нет
- Coso Erm 2017Документ11 страницCoso Erm 2017RAFAEL MOTAVITAОценок пока нет
- HM Treasury Risk Management Assessment FrameworkДокумент22 страницыHM Treasury Risk Management Assessment FrameworkAndy TrederОценок пока нет
- How Is Risk AssessmentДокумент94 страницыHow Is Risk AssessmentDung NguyenОценок пока нет
- Ey Shifting Focus Risk Culture at The Forefront of BankingДокумент86 страницEy Shifting Focus Risk Culture at The Forefront of BankingChristian AquinoОценок пока нет
- Corruption Bibliography 2015Документ307 страницCorruption Bibliography 2015api-290917515Оценок пока нет
- Achieving Excellence Guide Risk & Value ManagementДокумент24 страницыAchieving Excellence Guide Risk & Value ManagementsizwehОценок пока нет
- Use Risk Impact/Probability Chart Manage ICT Congress RisksДокумент2 страницыUse Risk Impact/Probability Chart Manage ICT Congress RisksJonathanA.RamirezОценок пока нет
- Window Merchandising Functions TitleДокумент131 страницаWindow Merchandising Functions TitlechankiiОценок пока нет
- Inherent and Control Risk FactorsДокумент9 страницInherent and Control Risk FactorsSaur MaruliОценок пока нет
- Key Risk IndicatorДокумент3 страницыKey Risk IndicatorLuis MalaverОценок пока нет
- Factsheet: 3 Lines of Defence' Combined Assurance Model: Connect Support AdvanceДокумент2 страницыFactsheet: 3 Lines of Defence' Combined Assurance Model: Connect Support AdvanceWajdi AlissawiОценок пока нет
- Risk-Management-Guide-Cso-2010 - SampleДокумент17 страницRisk-Management-Guide-Cso-2010 - SampleJohnson Joshiraj Paul JeyarajОценок пока нет
- Internal Controls Survey Report 2018Документ24 страницыInternal Controls Survey Report 2018kunal butolaОценок пока нет
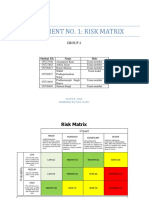
- EPM 2102.assignment 1. Group-4Документ8 страницEPM 2102.assignment 1. Group-4Satnam SinghОценок пока нет
- ERM PresentationДокумент13 страницERM PresentationBhargav Rishabh BaruahОценок пока нет
- COSO Framework - September 2012Документ166 страницCOSO Framework - September 2012Nawsher21Оценок пока нет
- MBAXGBAT9130 Enterprise Risk Management Overview Session 3 2017 PDFДокумент38 страницMBAXGBAT9130 Enterprise Risk Management Overview Session 3 2017 PDFmbs mbaОценок пока нет
- 01 Robert Conti Lean Production Job Stress 0240260904Документ26 страниц01 Robert Conti Lean Production Job Stress 0240260904Lisa Anggun SaraswatiОценок пока нет
- Final SMS - Orlando - Session 3101 FinalДокумент28 страницFinal SMS - Orlando - Session 3101 FinalDavidÉmileDurkheimОценок пока нет
- Operational Risk ManagementДокумент115 страницOperational Risk ManagementberiОценок пока нет
- Monetary Policies and Independence of The Central Banks in E7 CountriesДокумент79 страницMonetary Policies and Independence of The Central Banks in E7 CountriesFahri RifqiОценок пока нет
- Risk Management in E-BusinessДокумент5 страницRisk Management in E-BusinessTharindu ChathurangaОценок пока нет
- Enterprise Risk Management QuestionnaireДокумент4 страницыEnterprise Risk Management QuestionnaireirfanОценок пока нет
- Risk Management System for ABCДокумент25 страницRisk Management System for ABClizasaari100% (3)
- 4 - COSO ERM and More - Protiviti - Bob HirthДокумент70 страниц4 - COSO ERM and More - Protiviti - Bob HirthRena Rose MalunesОценок пока нет
- 2012 Compliance StudyДокумент24 страницы2012 Compliance StudyMarc BohnОценок пока нет
- Business Continuity Management Keeping The Wheels in Motion - AusGovДокумент111 страницBusiness Continuity Management Keeping The Wheels in Motion - AusGovMichael RogersОценок пока нет
- Co So Enterprise Risk Management FrameworkДокумент2 страницыCo So Enterprise Risk Management FrameworkasifsubhanОценок пока нет
- COSO Executive SummaryДокумент5 страницCOSO Executive SummaryabekaforumОценок пока нет
- Ey Insurance Maintaining Internal Controls and Trust While Remote Working During Covid 19Документ11 страницEy Insurance Maintaining Internal Controls and Trust While Remote Working During Covid 19Arun RajanОценок пока нет
- Business Continuity Planning (BCP) & Disaster Recovery Planning (DRP)Документ33 страницыBusiness Continuity Planning (BCP) & Disaster Recovery Planning (DRP)eriquew100% (1)
- Auditing in Times of Social Distancing: The e Ffect of COVID-19 On Auditing QualityДокумент10 страницAuditing in Times of Social Distancing: The e Ffect of COVID-19 On Auditing Qualitymuhammad umerОценок пока нет
- Enterprise Risk Management - Integrated Framework: Applying COSO'sДокумент49 страницEnterprise Risk Management - Integrated Framework: Applying COSO'sTutu BazatuОценок пока нет
- Systems in Focus 0409Документ32 страницыSystems in Focus 0409ylaala8010Оценок пока нет
- Environmental Impact AssessmentДокумент22 страницыEnvironmental Impact AssessmentAditya R. PadhiОценок пока нет
- Auditor Perceptions of Audit Workloads Audit Quality and Job SasticfationДокумент43 страницыAuditor Perceptions of Audit Workloads Audit Quality and Job SasticfationKevin PhạmОценок пока нет
- 04RM - Risk-Assessment 2Документ32 страницы04RM - Risk-Assessment 2Darren TanОценок пока нет
- Risk MGMTДокумент10 страницRisk MGMTcuteleo23Оценок пока нет
- How integrity due diligence protects companies from risksДокумент17 страницHow integrity due diligence protects companies from risksNikhil Jain100% (1)
- Human Error and Models of BehaviourДокумент46 страницHuman Error and Models of BehaviourWilliam WongОценок пока нет
- A Structured Approach To Building Predictive Key Risk IndicatorsДокумент6 страницA Structured Approach To Building Predictive Key Risk IndicatorsmbelgedeshuОценок пока нет
- Risk Management Framework System Development GuidelinesДокумент14 страницRisk Management Framework System Development Guidelinesعبدالمعز المليانОценок пока нет
- Risk Management Study CaseДокумент6 страницRisk Management Study CaseDevina AninditaОценок пока нет
- Erm Coso PDFДокумент2 страницыErm Coso PDFLindsay0% (1)
- White Paper Combined AssuranceДокумент11 страницWhite Paper Combined Assurancewdr80Оценок пока нет
- IAA Risk Book Chapter 4 - Operational Risk Peter Boller Caroline Grégoire Toshihiro Kawano Executive SummaryДокумент17 страницIAA Risk Book Chapter 4 - Operational Risk Peter Boller Caroline Grégoire Toshihiro Kawano Executive SummaryAlexanderHFFОценок пока нет
- Ramp Safety CultureДокумент11 страницRamp Safety CultureRumesh ThilakarathnaОценок пока нет
- IIA-CFSA exam questions and answersДокумент202 страницыIIA-CFSA exam questions and answersRahib JaskaniОценок пока нет
- Guidance On Conducting Environment Audit PDFДокумент71 страницаGuidance On Conducting Environment Audit PDFShane RodriguezОценок пока нет
- How To Manage Regulatory RiskДокумент3 страницыHow To Manage Regulatory Riskk3wlm3Оценок пока нет
- Ior Kri Event Slides AcДокумент15 страницIor Kri Event Slides AcAnonymous iMq2HDvVqОценок пока нет
- Aligning Risk With Strategy and PerformanceДокумент9 страницAligning Risk With Strategy and PerformancemajowkaОценок пока нет
- A Practitioner's Guide to Effective Maritime and Port SecurityОт EverandA Practitioner's Guide to Effective Maritime and Port SecurityОценок пока нет
- Bump Caps Vs Hard HatsДокумент6 страницBump Caps Vs Hard HatsAnonymous ocCa18RОценок пока нет
- Assesing The Need of PpeДокумент57 страницAssesing The Need of PpeAli AkbarОценок пока нет
- Egress Fire LPДокумент4 страницыEgress Fire LPRobert Paredes DimapilisОценок пока нет
- Working at Heights GuidelineДокумент13 страницWorking at Heights GuidelineKwang Sun100% (1)
- Contractor Job Safety PlanДокумент15 страницContractor Job Safety PlanAnonymous ocCa18RОценок пока нет
- 8d Training 9-8-2008-Root Cause AnalysisДокумент78 страниц8d Training 9-8-2008-Root Cause AnalysisShashindra Dhopeshwar100% (1)
- Thermal Cold Stress RiskДокумент4 страницыThermal Cold Stress Riskted_connellОценок пока нет
- Electrical HazardsДокумент26 страницElectrical HazardsAnonymous ocCa18RОценок пока нет
- Top 10 Property Fire HazardsДокумент4 страницыTop 10 Property Fire HazardsAnonymous ocCa18RОценок пока нет
- Ehs Guidance For Contractors: Wellesley CollegeДокумент2 страницыEhs Guidance For Contractors: Wellesley CollegeAnonymous ocCa18RОценок пока нет
- HSG 65 Guide To Measuring H&S Performance 2002Документ30 страницHSG 65 Guide To Measuring H&S Performance 2002venapusaОценок пока нет
- Solvent Recovery and VOC Emission Control SystemsДокумент8 страницSolvent Recovery and VOC Emission Control SystemsAnonymous ocCa18RОценок пока нет
- 8 Managing Process ChangesДокумент30 страниц8 Managing Process ChangesAnonymous ocCa18RОценок пока нет
- Breaking Containment - Process Cleaning Operations PDFДокумент4 страницыBreaking Containment - Process Cleaning Operations PDFAnonymous ocCa18RОценок пока нет
- Safety Audit in Developing CountriesДокумент8 страницSafety Audit in Developing CountriesAnonymous ocCa18RОценок пока нет
- Ageing Plant Summary GuideДокумент53 страницыAgeing Plant Summary GuideEyoma EtimОценок пока нет
- Ageing Plant Summary GuideДокумент53 страницыAgeing Plant Summary GuideEyoma EtimОценок пока нет
- Compressed Air SafetyДокумент9 страницCompressed Air SafetyAnonymous ocCa18RОценок пока нет
- Behavior Based Safety ManagementДокумент4 страницыBehavior Based Safety ManagementAnonymous ocCa18R100% (1)
- Occupational Exposure AssessmentДокумент59 страницOccupational Exposure AssessmentAnonymous ocCa18RОценок пока нет
- Nitrogen BlanketingДокумент7 страницNitrogen Blanketing3bandhuОценок пока нет
- Size of Access Openings in Boilers and Pressure VesselsДокумент3 страницыSize of Access Openings in Boilers and Pressure VesselsAnonymous ocCa18RОценок пока нет
- Divinylbenzene Storage and HandlingДокумент8 страницDivinylbenzene Storage and HandlingAnonymous ocCa18RОценок пока нет
- Process Safety Enhancement in Chemical Plant Design by Exploiting Accident KnowledgeДокумент88 страницProcess Safety Enhancement in Chemical Plant Design by Exploiting Accident KnowledgeAnonymous ocCa18RОценок пока нет
- Prohibiting Wooden Pallets For Hydrogen Peroxide H2O2 DrumsДокумент2 страницыProhibiting Wooden Pallets For Hydrogen Peroxide H2O2 DrumsAnonymous ocCa18RОценок пока нет
- Double Block and Bleed ValvesДокумент1 страницаDouble Block and Bleed ValvesAnonymous ocCa18RОценок пока нет
- D BB Pipeline Isolation PaperДокумент24 страницыD BB Pipeline Isolation Paperhadi137Оценок пока нет
- Space Analysis in Orthodontic: University of GlasgowДокумент16 страницSpace Analysis in Orthodontic: University of GlasgowNizam Muhamad100% (1)
- Live Performance Award Ma000081 Pay GuideДокумент48 страницLive Performance Award Ma000081 Pay GuideDan LijndersОценок пока нет
- 50-Orthodontic Objectives in Orthognathic Surgery-State of The PDFДокумент15 страниц50-Orthodontic Objectives in Orthognathic Surgery-State of The PDFDeena A. AlshwairikhОценок пока нет
- TDS Versimax HD4 15W40Документ1 страницаTDS Versimax HD4 15W40Amaraa DОценок пока нет
- Frank Wood S Business Accounting 1Документ13 страницFrank Wood S Business Accounting 1Kofi AsaaseОценок пока нет
- Genetically Engineered MicroorganismsДокумент6 страницGenetically Engineered Microorganismsaishwarya joshiОценок пока нет
- Reach Out and Read Georgia Selected For AJC Peachtree Road Race Charity Partner ProgramДокумент2 страницыReach Out and Read Georgia Selected For AJC Peachtree Road Race Charity Partner ProgramPR.comОценок пока нет
- Valvula de Leve MasterДокумент20 страницValvula de Leve Masterguillermo trejosОценок пока нет
- PERSONS Finals Reviewer Chi 0809Документ153 страницыPERSONS Finals Reviewer Chi 0809Erika Angela GalceranОценок пока нет
- SM RSJ 420 800Документ77 страницSM RSJ 420 800elshan_asgarovОценок пока нет
- Very Easy Toeic Units 7 - 12 (Q1)Документ39 страницVery Easy Toeic Units 7 - 12 (Q1)Minh KhaiОценок пока нет
- A&P 2 - Digestive System Flashcards - QuizletДокумент1 страницаA&P 2 - Digestive System Flashcards - QuizletMunachande KanondoОценок пока нет
- Workplace Hazard Analysis ProcedureДокумент12 страницWorkplace Hazard Analysis ProcedureKent Nabz60% (5)
- UNICESS KR Consmetics Maeteria Nunssupjara 01apr23Документ44 страницыUNICESS KR Consmetics Maeteria Nunssupjara 01apr23ZB ChuaОценок пока нет
- Construction and Operation 1. Air Conditioning Control PanelДокумент18 страницConstruction and Operation 1. Air Conditioning Control PanelRoma KuzmychОценок пока нет
- Theories of Motivation and Child Moral DevelopmentДокумент5 страницTheories of Motivation and Child Moral DevelopmentPamela mirandaОценок пока нет
- Growing Turmeric: Keys To SuccessДокумент4 страницыGrowing Turmeric: Keys To SuccessAnkit ShahОценок пока нет
- Apc 8x Install Config Guide - rn0 - LT - enДокумент162 страницыApc 8x Install Config Guide - rn0 - LT - enOney Enrique Mendez MercadoОценок пока нет
- Mufon Ufo JournalДокумент21 страницаMufon Ufo JournalSAB78Оценок пока нет
- Piping Material Classes GuideДокумент98 страницPiping Material Classes GuideLuis Pottozen VillanuevaОценок пока нет
- Ucg200 12Документ3 страницыUcg200 12ArielОценок пока нет
- Quality Control Plan Static EquipmentДокумент1 страницаQuality Control Plan Static EquipmentdhasdjОценок пока нет
- Ensure Even Preload with Proper Tightening Tools and SequenceДокумент2 страницыEnsure Even Preload with Proper Tightening Tools and SequenceMachineryengОценок пока нет
- Steam System Design RequirementsДокумент29 страницSteam System Design RequirementsAthirahОценок пока нет
- 07 Chapter2Документ16 страниц07 Chapter2Jigar JaniОценок пока нет
- Female Reproductive System Histology IДокумент5 страницFemale Reproductive System Histology ISolomon Seth SallforsОценок пока нет
- C. Drug Action 1Документ28 страницC. Drug Action 1Jay Eamon Reyes MendrosОценок пока нет
- BS 5911-120Документ33 страницыBS 5911-120Niranjan GargОценок пока нет
- Impact of Covid-19 On Audit Quality: Presented byДокумент13 страницImpact of Covid-19 On Audit Quality: Presented byMST. SADIYA SULTANAОценок пока нет
- HierbasДокумент25 страницHierbasrincón de la iohОценок пока нет