Вам также может понравиться
- Sjogren Syndrome A Case ReportДокумент3 страницыSjogren Syndrome A Case ReportEditor IJTSRDОценок пока нет
- Jurnal BM DittaДокумент4 страницыJurnal BM DittaRyans FkdokgiОценок пока нет
- Case Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisДокумент5 страницCase Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDjumadi AkbarОценок пока нет
- Igg4-Related Disease: An Orphan Disease With Many Faces: Review Open AccessДокумент14 страницIgg4-Related Disease: An Orphan Disease With Many Faces: Review Open Accessmiguel roldanОценок пока нет
- 329-Article Text-1006-2-10-20200429Документ5 страниц329-Article Text-1006-2-10-20200429Drina PaglinawanОценок пока нет
- EN + EosinofiliaДокумент3 страницыEN + EosinofiliaAna Flavia BaptistaОценок пока нет
- Tubercular ScleritisДокумент5 страницTubercular Scleritismutya yulindaОценок пока нет
- tmp3045 TMPДокумент4 страницыtmp3045 TMPFrontiersОценок пока нет
- MainДокумент3 страницыMainderkha SajОценок пока нет
- Oral Findings of Systemic Lupus Erythematosus - A Grand Round CaseДокумент6 страницOral Findings of Systemic Lupus Erythematosus - A Grand Round CaseArditya Dwi YudistiraОценок пока нет
- Herpes Ophthalmicus: Review: ZosterДокумент4 страницыHerpes Ophthalmicus: Review: ZosterAndika Wahyu UtomoОценок пока нет
- A Rare Case of Tubercular Pansinusitis With Orbital and Intracranial ExtensionДокумент3 страницыA Rare Case of Tubercular Pansinusitis With Orbital and Intracranial Extensionnajmarani devi firdausОценок пока нет
- 11 194scleroderma A Case ReportДокумент3 страницы11 194scleroderma A Case ReportAfiatul MukarromahОценок пока нет
- Infectious Mononucleosis: A Case ReportДокумент3 страницыInfectious Mononucleosis: A Case ReportSerghei CojocariОценок пока нет
- Review 01-06 PDFДокумент6 страницReview 01-06 PDFEditor IjprtОценок пока нет
- CRM 2015Документ7 страницCRM 2015Kiran KumarОценок пока нет
- Somorin SsДокумент8 страницSomorin SsChikezie OnwukweОценок пока нет
- Rosai Dorfman ChildДокумент3 страницыRosai Dorfman ChildElena PoriazovaОценок пока нет
- Sjögren's SyndromeДокумент18 страницSjögren's Syndromezakaria dbanОценок пока нет
- Lepromatous Leprosy in Erythema Nodosum Leprosum Reaction Mimicking Sweet's SyndromeДокумент2 страницыLepromatous Leprosy in Erythema Nodosum Leprosum Reaction Mimicking Sweet's SyndromeAstri MelistriОценок пока нет
- Submandibular Gland Chronic Sialadenitis: A Case ReportДокумент3 страницыSubmandibular Gland Chronic Sialadenitis: A Case Reportaprilia rizqiОценок пока нет
- Oral Findings of Systemic Lupus Erythematosus-A Grand Round CaseДокумент5 страницOral Findings of Systemic Lupus Erythematosus-A Grand Round CaseIntanОценок пока нет
- Lupus Vulgaris of External NoseДокумент3 страницыLupus Vulgaris of External NosejalalfaizОценок пока нет
- Practice: Kikuchi-Fujimoto Disease: Lymphadenopathy in SiblingsДокумент4 страницыPractice: Kikuchi-Fujimoto Disease: Lymphadenopathy in SiblingsBobby Faisyal RakhmanОценок пока нет
- Iaet 12 I 2 P 135Документ2 страницыIaet 12 I 2 P 135leonjunchan_66965707Оценок пока нет
- Gradenigo's Syndrome - A Rare Case Report: Medical SciencesДокумент2 страницыGradenigo's Syndrome - A Rare Case Report: Medical SciencesSODAZZZAОценок пока нет
- Diagnosis in OncologyДокумент22 страницыDiagnosis in OncologyAndi SuryajayaОценок пока нет
- Hypereosinophilic Syndrome: C. Venkatesh, E. Mahender, S. Janani, S. MalathiДокумент3 страницыHypereosinophilic Syndrome: C. Venkatesh, E. Mahender, S. Janani, S. MalathialaaОценок пока нет
- Clin Infect Dis. 1996 Eriksson 1091 8Документ8 страницClin Infect Dis. 1996 Eriksson 1091 8zul090Оценок пока нет
- Plasmacytoma of The Thyroid Gland: Case Report and Review of The LiteratureДокумент10 страницPlasmacytoma of The Thyroid Gland: Case Report and Review of The Literaturedede wawaОценок пока нет
- Case Report: Subcorneal Pustular Dermatosis in Childhood: A Case Report and Review of The LiteratureДокумент6 страницCase Report: Subcorneal Pustular Dermatosis in Childhood: A Case Report and Review of The LiteratureIrsalinaHusnaAzwirОценок пока нет
- Yayli (2013) - NS Resembles KaposiДокумент3 страницыYayli (2013) - NS Resembles KaposiIlma ArifaniОценок пока нет
- Otogenic Brain Abscess Our ExperienceДокумент5 страницOtogenic Brain Abscess Our ExperienceNeysaAzaliaEfrimaisaОценок пока нет
- Coexistence of Cutaneous Tuberculosis (Scrofuloderma) and Hanseniasis-A Rare PresentationДокумент2 страницыCoexistence of Cutaneous Tuberculosis (Scrofuloderma) and Hanseniasis-A Rare PresentationGesza Utama PutraОценок пока нет
- Ophthal Notes PGДокумент6 страницOphthal Notes PGSwati TyagiОценок пока нет
- 1 s2.0 S2173573514000490 MainДокумент2 страницы1 s2.0 S2173573514000490 MainHerryAsu-songkoОценок пока нет
- Soldiers From Indo Myanmar Border Presenting With Scrub Typhus: Case ReportДокумент5 страницSoldiers From Indo Myanmar Border Presenting With Scrub Typhus: Case ReportIOSRjournalОценок пока нет
- Malignant Otitis ExternaДокумент5 страницMalignant Otitis Externasergeantchai068Оценок пока нет
- SarcoidosisДокумент59 страницSarcoidosisMaria Dodon100% (2)
- Dental Journal: Oral Lesions As A Clinical Sign of Systemic Lupus ErythematosusДокумент6 страницDental Journal: Oral Lesions As A Clinical Sign of Systemic Lupus ErythematosusIin Ardi AОценок пока нет
- Ocular Adnexal and Orbital Amyloidosis: A Case Series and Literature ReviewДокумент18 страницOcular Adnexal and Orbital Amyloidosis: A Case Series and Literature ReviewMariela LezamaОценок пока нет
- SMW 10050Документ8 страницSMW 10050lapulga10Оценок пока нет
- 1793-Article Text-19545-2-10-20190508 PDFДокумент5 страниц1793-Article Text-19545-2-10-20190508 PDFRezkyRamadhaniSyarifОценок пока нет
- 33 Shumez EtalДокумент4 страницы33 Shumez EtaleditorijmrhsОценок пока нет
- Stemming The Outbreak: SyphilisДокумент7 страницStemming The Outbreak: SyphilisamimusriОценок пока нет
- Complications of Suppurative Otitis Media: Still A Problem in The 21st CenturyДокумент7 страницComplications of Suppurative Otitis Media: Still A Problem in The 21st CenturyNisa SulistiaОценок пока нет
- Gorlin Syndrom SSDC.Документ3 страницыGorlin Syndrom SSDC.HarjotBrarОценок пока нет
- Etiology of Proptosis in Children Sindhu 1998Документ3 страницыEtiology of Proptosis in Children Sindhu 1998Putri Wulan SukmawatiОценок пока нет
- Efficacy of Homoeopathy in Treatment of Sarcoidosis 50 CasesДокумент32 страницыEfficacy of Homoeopathy in Treatment of Sarcoidosis 50 CasesDr. Rajneesh Kumar Sharma MD Hom100% (1)
- ANA TestДокумент9 страницANA TestNena_mileyОценок пока нет
- Descricion ofДокумент5 страницDescricion ofLlrss AdnОценок пока нет
- Preseptal and Orbital Cellulitis: A 10-Year Review of Hospitalized PatientsДокумент8 страницPreseptal and Orbital Cellulitis: A 10-Year Review of Hospitalized PatientsApril MitchellОценок пока нет
- Scurvy Masquerading As Juvenile Idiopathic Arthritis or VasculitisДокумент6 страницScurvy Masquerading As Juvenile Idiopathic Arthritis or VasculitisZach Segmuel MiñanoОценок пока нет
- Lethal Midline Granuloma Importance of Early Diagnosis: A Case ReportДокумент0 страницLethal Midline Granuloma Importance of Early Diagnosis: A Case ReportdeolukmanaОценок пока нет
- Ecthyma Contagiosum (Human Orf)Документ2 страницыEcthyma Contagiosum (Human Orf)Deba P SarmaОценок пока нет
- Eosinophilic Granuloma of The Mandible in A Four Year Old Boy A Rare Case Report and Review of Literature Joccr 3 1061Документ4 страницыEosinophilic Granuloma of The Mandible in A Four Year Old Boy A Rare Case Report and Review of Literature Joccr 3 1061Paolo MaldinicerutiОценок пока нет
- Sinonasal Eosinophilic Angiocentric FibrosisДокумент10 страницSinonasal Eosinophilic Angiocentric FibrosisPriskila Marlen YoltuwuОценок пока нет
- Case Report Acute Idiopathic Scrotal Edema MILMED-D-13-00103Документ3 страницыCase Report Acute Idiopathic Scrotal Edema MILMED-D-13-00103YJanitorОценок пока нет
- Dental Sealant ToxicityДокумент14 страницDental Sealant ToxicityGuru SvamiОценок пока нет
- Heart Valve Disease: State of the ArtОт EverandHeart Valve Disease: State of the ArtJose ZamoranoОценок пока нет
- The Learning Principle PRINTДокумент5 страницThe Learning Principle PRINTnurulОценок пока нет
- BOQ New Store Plumbing MДокумент10 страницBOQ New Store Plumbing MMd. Mominul IslamОценок пока нет
- Combat Patrol - GREY KNIGHTSДокумент6 страницCombat Patrol - GREY KNIGHTSJan PolisiakОценок пока нет
- PREQ3-1 Shrouded VisionsДокумент47 страницPREQ3-1 Shrouded VisionsVelenar ShadowalkerОценок пока нет
- 74HC4049Документ11 страниц74HC4049jnax101Оценок пока нет
- Lab-Journal Compiler ConstructionДокумент20 страницLab-Journal Compiler ConstructionAbdullah ArshadОценок пока нет
- 060610at617pm Mayday Re Are We Under Terrorist Attack YesДокумент12 страниц060610at617pm Mayday Re Are We Under Terrorist Attack YesRalph Charles Whitley, Sr.Оценок пока нет
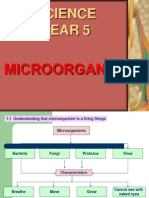
- Science Year 5: MicroorganismsДокумент8 страницScience Year 5: MicroorganismscthanifahОценок пока нет
- Machine Elements in Mechanical Design Solution PDFДокумент309 страницMachine Elements in Mechanical Design Solution PDFazkonaОценок пока нет
- Gun TypesДокумент125 страницGun Typesdewaaaaa-76100% (2)
- Ethics and Social Responsibilities of Entrepreneurship PDFДокумент4 страницыEthics and Social Responsibilities of Entrepreneurship PDFRevuru ArunaОценок пока нет
- Lesson Plan On Transport MechanismsДокумент5 страницLesson Plan On Transport Mechanismsjecel taray100% (4)
- Practice UA3 Spring 2023Документ15 страницPractice UA3 Spring 2023moyin idowuОценок пока нет
- DefinitionsДокумент7 страницDefinitionsJazmine ButuhanОценок пока нет
- Algorithm and FlowchartsДокумент9 страницAlgorithm and FlowchartsNambashisha RyngksaiОценок пока нет
- Chapter 5. Elementary ProbabilityДокумент11 страницChapter 5. Elementary ProbabilityyonasОценок пока нет
- Guard Rail Cataloge PDFДокумент28 страницGuard Rail Cataloge PDFreza acbariОценок пока нет
- AttentionДокумент26 страницAttentionKarn KunteОценок пока нет
- Youth Protection WaiverДокумент1 страницаYouth Protection WaiverKatie McCarthyОценок пока нет
- The Metal Oxide FETДокумент7 страницThe Metal Oxide FETSitty GuОценок пока нет
- How To Write Master Thesis AbstractДокумент8 страницHow To Write Master Thesis Abstractidmcgzbaf100% (2)
- Ritter Insurance Broker PresentationДокумент10 страницRitter Insurance Broker Presentationritter.roОценок пока нет
- Tài liệu tiếng Trung HSK5Документ1 страницаTài liệu tiếng Trung HSK5Nguyễn Ngọc Xuân NghiêmОценок пока нет
- ModelsДокумент6 страницModelsUJJWALОценок пока нет
- Noc20-Cs53 Week 04 Assignment 02Документ4 страницыNoc20-Cs53 Week 04 Assignment 02Modicare QuiteОценок пока нет
- Lecture 06 - Types of Permanent Mold Casting ProcessesДокумент26 страницLecture 06 - Types of Permanent Mold Casting ProcessesThe NoobОценок пока нет
- Soalan Tugasan 2 HBEC4403 OUMДокумент7 страницSoalan Tugasan 2 HBEC4403 OUMTutor EvonОценок пока нет
- IBS Site Survey ReportДокумент101 страницаIBS Site Survey ReportSyed Zahid ShahОценок пока нет
- Documents and Data RequirementsДокумент2 страницыDocuments and Data RequirementsGerardo Leon RoblesОценок пока нет
- Formal Declarative EndingДокумент13 страницFormal Declarative EndingMary Mariette EscalanteОценок пока нет