Вам также может понравиться
- Measuring Our Safety-Ness: by David Carr Director of SafetyДокумент4 страницыMeasuring Our Safety-Ness: by David Carr Director of SafetyrotorbrentОценок пока нет
- TAC Attack October 1961Документ20 страницTAC Attack October 1961TateОценок пока нет
- ASRS CALLBACK Issue 506 - March 2022Документ2 страницыASRS CALLBACK Issue 506 - March 2022François Hubert SergiОценок пока нет
- February - Stevedore Injured by TwistlockДокумент2 страницыFebruary - Stevedore Injured by TwistlockHarman SandhuОценок пока нет
- Positive Vision: Enjoying the Adventures and Advantages of Poor EyesightОт EverandPositive Vision: Enjoying the Adventures and Advantages of Poor EyesightОценок пока нет
- Aviation EnglishДокумент86 страницAviation Englishtmhoangvna100% (1)
- The Decision Was Easy: The Ground Truth About Safety LeadershipОт EverandThe Decision Was Easy: The Ground Truth About Safety LeadershipОценок пока нет
- Contingency PlanДокумент2 страницыContingency Planapi-630394298Оценок пока нет
- Near Miss Toolbox TalkДокумент2 страницыNear Miss Toolbox Talkpruncu.alianmОценок пока нет
- Callback - NASA - 492Документ2 страницыCallback - NASA - 492Αλέξανδρος ΒασιλειάδηςОценок пока нет
- Urban Survival Guide Top Urban Survival Skills (Field & Stream) (2012) PDFДокумент11 страницUrban Survival Guide Top Urban Survival Skills (Field & Stream) (2012) PDF20180321Оценок пока нет
- Haunter Grey Deception, Seven Book Boxed Set: Includes Upheaval, Evolution, and the PrequelsОт EverandHaunter Grey Deception, Seven Book Boxed Set: Includes Upheaval, Evolution, and the PrequelsОценок пока нет
- Hazard HeroДокумент31 страницаHazard HeroKennet PhanОценок пока нет
- 005 - Vocabulary - Taking OffДокумент3 страницы005 - Vocabulary - Taking OffFábia RodriguesОценок пока нет
- Safety Awareness: Celebrating Operational ExcellenceДокумент8 страницSafety Awareness: Celebrating Operational ExcellenceMario AndrewОценок пока нет
- The Secret Nuclear Threat: Trident Whistleblower William McneillyДокумент17 страницThe Secret Nuclear Threat: Trident Whistleblower William McneillyLeakSourceInfoОценок пока нет
- English Writers Effect InsДокумент4 страницыEnglish Writers Effect InsChunky PresidentОценок пока нет
- HalflifeДокумент13 страницHalflifeRooWWОценок пока нет
- "To Err Is Human ": AccountabilityДокумент4 страницы"To Err Is Human ": AccountabilityrotorbrentОценок пока нет
- (Sample Essay) (Hope)Документ2 страницы(Sample Essay) (Hope)muhdsabri51Оценок пока нет
- Critical Thinking in Company 3.0 Lesson 2015Документ3 страницыCritical Thinking in Company 3.0 Lesson 2015Jimmy HaddadОценок пока нет
- Material para Estudos Da AVI Azul Linhas AéreasДокумент32 страницыMaterial para Estudos Da AVI Azul Linhas AéreasThaís BaraúnaОценок пока нет
- Student Guide 9: Activity 1 1.1 Explain The Meaning of The Following WordsДокумент9 страницStudent Guide 9: Activity 1 1.1 Explain The Meaning of The Following WordsLORAINE CAUSADO BARONОценок пока нет
- Blind Suctioning For BeginnersДокумент7 страницBlind Suctioning For BeginnersMark HammerschmidtОценок пока нет
- Risk Management in ParaglidingДокумент2 страницыRisk Management in Paraglidinglinh nguyenОценок пока нет
- Crime Scene InvestigationДокумент94 страницыCrime Scene InvestigationTina SwainОценок пока нет
- The Practice or Art of Using Language With Fluency and AptnessДокумент1 страницаThe Practice or Art of Using Language With Fluency and AptnessCorey HomОценок пока нет
- David Fravor Statement For House Oversight CommitteeДокумент3 страницыDavid Fravor Statement For House Oversight CommitteeStephanie Dube DwilsonОценок пока нет
- English (101-103)Документ5 страницEnglish (101-103)Umiyanti AzizahОценок пока нет
- Filename(s) Quote Play: Absolutely. Menu 0:00Документ17 страницFilename(s) Quote Play: Absolutely. Menu 0:00uwaifotonyОценок пока нет
- Ladies and Gentlemen IДокумент1 страницаLadies and Gentlemen IPanergo ErickajoyОценок пока нет
- Risk Assesment HGДокумент3 страницыRisk Assesment HGapi-632030001Оценок пока нет
- Oldier Onors Rogram and Ospital With Riceless Ift: S H P H P GДокумент8 страницOldier Onors Rogram and Ospital With Riceless Ift: S H P H P GrotorbrentОценок пока нет
- The Worst-Case Scenario Survival Handbook: TravelОт EverandThe Worst-Case Scenario Survival Handbook: TravelРейтинг: 3.5 из 5 звезд3.5/5 (346)
- Safety Compass March 2014Документ5 страницSafety Compass March 2014rotorbrentОценок пока нет
- KLBB Rnav (GPS) 35lДокумент1 страницаKLBB Rnav (GPS) 35lrotorbrentОценок пока нет
- "How To Murphy-Proof Your Life": If Anything Can Go Wrong, It WillДокумент4 страницы"How To Murphy-Proof Your Life": If Anything Can Go Wrong, It WillrotorbrentОценок пока нет
- "How To Murphy-Proof Your Life": If Anything Can Go Wrong, It WillДокумент4 страницы"How To Murphy-Proof Your Life": If Anything Can Go Wrong, It WillrotorbrentОценок пока нет
- "To Err Is Human ": AccountabilityДокумент4 страницы"To Err Is Human ": AccountabilityrotorbrentОценок пока нет
- G500 Cockpit Reference GuideДокумент84 страницыG500 Cockpit Reference Guiderotorbrent100% (1)
- Tradition Meet Practical DriftДокумент6 страницTradition Meet Practical DriftrotorbrentОценок пока нет
- "Sugar N Spice ": - One of These Is Not Like The Other (Part I)Документ5 страниц"Sugar N Spice ": - One of These Is Not Like The Other (Part I)rotorbrentОценок пока нет
- Trimble 2101 ManualДокумент243 страницыTrimble 2101 ManualrotorbrentОценок пока нет
- The Dutch Oven CookbookДокумент53 страницыThe Dutch Oven CookbookCrisОценок пока нет
- School Rules and Policy Manual: ArcproДокумент13 страницSchool Rules and Policy Manual: ArcprorotorbrentОценок пока нет
- Book of EnochДокумент77 страницBook of EnochrotorbrentОценок пока нет
- Electric Motor Test RepairДокумент160 страницElectric Motor Test Repairrotorbrent100% (2)
- How To Make Professional Lock Pick ToolsДокумент5 страницHow To Make Professional Lock Pick Toolsvinekm6100% (6)
- Locksport International GuideДокумент22 страницыLocksport International Guidewhistjenn100% (2)
- Electric Motor Test RepairДокумент160 страницElectric Motor Test Repairrotorbrent100% (2)
- Coil Winding MachineДокумент4 страницыCoil Winding MachineJim90% (10)
- Skull Osteology & Cranial Cavity - TUSKДокумент66 страницSkull Osteology & Cranial Cavity - TUSKterima kasihОценок пока нет
- Installation Instructions: Lock-Down ScrewДокумент1 страницаInstallation Instructions: Lock-Down ScrewDhimas ZakariaОценок пока нет
- Tool Operating Manual Tool Operating Manual: 276-7273 Cylinder Sensor Test Box (In Cylinder Function Test)Документ12 страницTool Operating Manual Tool Operating Manual: 276-7273 Cylinder Sensor Test Box (In Cylinder Function Test)CarlosОценок пока нет
- Bed Bath MikeДокумент24 страницыBed Bath MikeMike100% (1)
- Surgical Site Infection (SSI) Event: Monthly Reporting PlanДокумент31 страницаSurgical Site Infection (SSI) Event: Monthly Reporting PlanDRMC InfectioncontrolserviceОценок пока нет
- 2090 2697 2 108 PDFДокумент5 страниц2090 2697 2 108 PDFMuhammad Riza FahlawiОценок пока нет
- Pelvis and Perineum (Appleton & Lange Review)Документ41 страницаPelvis and Perineum (Appleton & Lange Review)orea100% (2)
- Helix Alliance - Resume (Dr. Appukutty Manickam (Kumar) ) - 1Документ6 страницHelix Alliance - Resume (Dr. Appukutty Manickam (Kumar) ) - 1indo 5SОценок пока нет
- PE Theory Knowledge OrganiserДокумент5 страницPE Theory Knowledge OrganiserSharra LopezОценок пока нет
- Spinal Injury Nursing Care PlanДокумент2 страницыSpinal Injury Nursing Care PlanPatricia OrtegaОценок пока нет
- Fetal Macrosomia ArtДокумент14 страницFetal Macrosomia Artanyka2Оценок пока нет
- Chinese Herbal FormulasДокумент8 страницChinese Herbal Formulasryandakota100% (1)
- AORN Electrosurgery GuidelinesДокумент20 страницAORN Electrosurgery GuidelinesRudy DuterteОценок пока нет
- JZ990D43501 eДокумент6 страницJZ990D43501 eМаксим ПасичникОценок пока нет
- Scorebuilders 3Документ40 страницScorebuilders 3DeepRamanОценок пока нет
- D 100394 X 012Документ52 страницыD 100394 X 012Preyas SuvarnaОценок пока нет
- Jackson V AEG Live Transcripts of DR Scott David Saunders (Doctor)Документ69 страницJackson V AEG Live Transcripts of DR Scott David Saunders (Doctor)TeamMichaelОценок пока нет
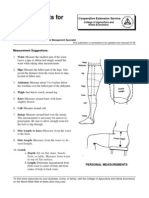
- Measurements For Fitting Pants: Guide C-209Документ2 страницыMeasurements For Fitting Pants: Guide C-209Ranil Hashan FОценок пока нет
- Vertebral Column Skull Projection MethodДокумент8 страницVertebral Column Skull Projection MethodLaFranz CabotajeОценок пока нет
- Shipboard High VoltageДокумент62 страницыShipboard High VoltageArun SОценок пока нет
- Radiographic Positioning and Radiologic Procedures I FinalsДокумент13 страницRadiographic Positioning and Radiologic Procedures I FinalsrozdhagaОценок пока нет
- Dorin The Dwarf SpellsДокумент3 страницыDorin The Dwarf Spellspotato123123aОценок пока нет
- Respiration PHYSIOДокумент23 страницыRespiration PHYSIOTauseef AfridiОценок пока нет
- Impaired Physical MobilityДокумент1 страницаImpaired Physical Mobilitykyaw100% (1)
- ARDSДокумент81 страницаARDSShanaz NovriandinaОценок пока нет
- Lucas vs. TuanoДокумент2 страницыLucas vs. Tuanomelinda elnarОценок пока нет
- A Fighter's Lines by Marzuki AliДокумент5 страницA Fighter's Lines by Marzuki AliAnonymous TADs3BevnОценок пока нет
- Accessory Navicular BoneДокумент29 страницAccessory Navicular BonePhysiotherapist AliОценок пока нет
- Article Review Kel 3 KompilasiДокумент21 страницаArticle Review Kel 3 KompilasiFazlin KhuzaimaОценок пока нет
- Safe Working ProcedureДокумент23 страницыSafe Working ProcedureBea MokОценок пока нет