Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- 1833 TX Melton, Daisy Mae DeathДокумент1 страница1833 TX Melton, Daisy Mae DeathRichard TonsingОценок пока нет
- Psychiatric Disability AssessmentДокумент19 страницPsychiatric Disability AssessmentDivya ThomasОценок пока нет
- Chapter 1Документ62 страницыChapter 1Ashenafi PaulosОценок пока нет
- The Pale Blood HuntДокумент92 страницыThe Pale Blood HuntRafael JunioОценок пока нет
- Hygienic Design Food IndustryДокумент19 страницHygienic Design Food IndustryLinaArev H100% (1)
- Field Visit PresentationДокумент33 страницыField Visit PresentationNib IndranilОценок пока нет
- Accessory TragusДокумент3 страницыAccessory TragusDeba P SarmaОценок пока нет
- Acantholytic Solar Keratosis, M 67, Forehead PDFДокумент6 страницAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaОценок пока нет
- Pilar Cyst With CrystalsДокумент2 страницыPilar Cyst With CrystalsDeba P SarmaОценок пока нет
- Acantholytic Bullous DiseaseДокумент4 страницыAcantholytic Bullous DiseaseDeba P SarmaОценок пока нет
- Acantholytic Dermatosis With DyskeratosisДокумент11 страницAcantholytic Dermatosis With DyskeratosisDeba P SarmaОценок пока нет
- Acantholytic Acanthoma. M 60, ScrotumДокумент8 страницAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaОценок пока нет
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Документ3 страницыAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaОценок пока нет
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Документ6 страницBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaОценок пока нет
- Results of Search in Google Scholar On 'Deba P Sarma'Документ28 страницResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaОценок пока нет
- Acantholytic Actinic KeratosisДокумент4 страницыAcantholytic Actinic KeratosisDeba P SarmaОценок пока нет
- Xanthogranuloma, M 30, Right ElbowДокумент4 страницыXanthogranuloma, M 30, Right ElbowDeba P SarmaОценок пока нет
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmДокумент7 страницXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaОценок пока нет
- Verruca Vulgaris., M 22.,PPTДокумент2 страницыVerruca Vulgaris., M 22.,PPTDeba P SarmaОценок пока нет
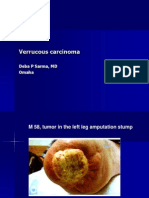
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpДокумент7 страницVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaОценок пока нет
- Xanthogranuloma PPT DSДокумент9 страницXanthogranuloma PPT DSDeba P SarmaОценок пока нет
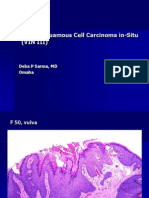
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaДокумент6 страницVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaОценок пока нет
- Verrucous Epidermal Nevus. F 43, ScalpДокумент4 страницыVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaОценок пока нет
- Verrucous Carcinoma of The Foot, M 63, Left FootДокумент8 страницVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- PQC-POL002 Qualification Guide For CertOH and iCertOH v1.0Документ25 страницPQC-POL002 Qualification Guide For CertOH and iCertOH v1.0Nathan MwewaОценок пока нет
- Top 10 Ranking Universities in West Africa 2022Документ1 страницаTop 10 Ranking Universities in West Africa 2022Bright OtchereОценок пока нет
- Periodontal AbscessДокумент27 страницPeriodontal AbscessAhmed Tawfig GamalОценок пока нет
- Promoting Smart Farming, Eco-Friendly and Innovative Technologies For Sustainable Coconut DevelopmentДокумент4 страницыPromoting Smart Farming, Eco-Friendly and Innovative Technologies For Sustainable Coconut DevelopmentMuhammad Maulana Sidik0% (1)
- MLC Lean Bronze Prep ClassДокумент2 страницыMLC Lean Bronze Prep ClassSalaОценок пока нет
- Philhealth Circular 013-2015Документ12 страницPhilhealth Circular 013-2015Kim Patrick DayosОценок пока нет
- Tumor AngiogenesisДокумент35 страницTumor AngiogenesisDoni Mirza KurniawanОценок пока нет
- Investigatory Project On Malaria: Name: M.Bhavya Class: XI C' Year: 2018 - 2019Документ18 страницInvestigatory Project On Malaria: Name: M.Bhavya Class: XI C' Year: 2018 - 2019Muramsetty Bhavya0% (1)
- The Warehouse Group Annual Report 2020Документ92 страницыThe Warehouse Group Annual Report 2020Meaza Kidusan ElhamОценок пока нет
- 11th Bio Zoology EM Official Answer Keys For Public Exam Mhay 2022 PDF DownloadДокумент3 страницы11th Bio Zoology EM Official Answer Keys For Public Exam Mhay 2022 PDF DownloadS. TAMIZHANОценок пока нет
- Clinico-Pathological Conference: Presented by The Department of Internal MedicineДокумент3 страницыClinico-Pathological Conference: Presented by The Department of Internal MedicineCloudy ClaudОценок пока нет
- Ciclul CardiacДокумент1 страницаCiclul CardiacAurelia AlexandraОценок пока нет
- Q3-Las-Health10-Module 3-Weeks 6-8Документ6 страницQ3-Las-Health10-Module 3-Weeks 6-8MA TEODORA CABEZADAОценок пока нет
- Final Thesis 22Документ66 страницFinal Thesis 22AdombireОценок пока нет
- Mapeh 2ND QДокумент5 страницMapeh 2ND QMaxicris SlowerОценок пока нет
- Ufgs 01 57 19.01 20Документ63 страницыUfgs 01 57 19.01 20jackcan501Оценок пока нет
- Pitbull StatementДокумент4 страницыPitbull StatementThe Citizen NewspaperОценок пока нет
- Case Group 1Документ10 страницCase Group 1JASMEEN RAVALОценок пока нет
- Wiley Veterinary GynaecologyДокумент2 страницыWiley Veterinary Gynaecologysanath0% (1)
- Experiment 4: Roadway Lighting Evaluation And: DesignДокумент12 страницExperiment 4: Roadway Lighting Evaluation And: DesignEdogawa ConanОценок пока нет
- Esmeron 10 MG/ML Solution For Injection Rocuronium Bromide Prescribing InformationДокумент3 страницыEsmeron 10 MG/ML Solution For Injection Rocuronium Bromide Prescribing InformationVeeta Ruchi LieОценок пока нет
- Acetylsalicylic AcidДокумент6 страницAcetylsalicylic AcidAdmin DownloadОценок пока нет
- School Form 8 sf8 Learner Basic Health and Nutrition Report AutomaticДокумент12 страницSchool Form 8 sf8 Learner Basic Health and Nutrition Report AutomaticKIRSTEN DIAZОценок пока нет
- BUPA Medical Service Providers Lebanon Updated-April 2013Документ3 страницыBUPA Medical Service Providers Lebanon Updated-April 2013gchaoul87Оценок пока нет