Вам также может понравиться
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- SalineДокумент6 страницSalinehamaadaОценок пока нет
- Rhesus PhenotypingДокумент3 страницыRhesus PhenotypinghamaadaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Cryoprecipitate: CompositionДокумент3 страницыCryoprecipitate: CompositionhamaadaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Special tests:) ١) ﺕﺎﻧﻮﺑﺮﻜﻴﺒﻟﺍ (Bicarbonate (Документ4 страницыSpecial tests:) ١) ﺕﺎﻧﻮﺑﺮﻜﻴﺒﻟﺍ (Bicarbonate (hamaadaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- 24 HR FFPДокумент4 страницы24 HR FFPhamaadaОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- ABO Grouping ProcedureДокумент2 страницыABO Grouping ProcedurehamaadaОценок пока нет
- Paked CellsДокумент3 страницыPaked CellshamaadaОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- NILAI UNIVERSITY COLLEGE DIPLOMA IN MEDICAL LABORATORY TECHNOLOGY PRACTICAL 5 WEAK D TESTINGДокумент2 страницыNILAI UNIVERSITY COLLEGE DIPLOMA IN MEDICAL LABORATORY TECHNOLOGY PRACTICAL 5 WEAK D TESTINGhamaadaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Home AДокумент11 страницHome AhamaadaОценок пока нет
- Cross-Matching: To Meet Wikipedia'sДокумент5 страницCross-Matching: To Meet Wikipedia'shamaadaОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- How To Use A BalanceДокумент1 страницаHow To Use A BalancehamaadaОценок пока нет
- Rhesus Grouping ProcedureДокумент1 страницаRhesus Grouping ProcedurehamaadaОценок пока нет
- Direct Antiglobulin Test (DAT)Документ2 страницыDirect Antiglobulin Test (DAT)hamaadaОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Immune ToleranceДокумент7 страницImmune TolerancehamaadaОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- ABO subgroups Bombay group phenotypesДокумент15 страницABO subgroups Bombay group phenotypeshamaadaОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Blood TherapyДокумент21 страницаBlood TherapySandra Ag Ariodere KeonyediОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Chitungwiza Central Hospital Laboratory DepartmentДокумент2 страницыChitungwiza Central Hospital Laboratory DepartmenthamaadaОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Antibody IdentificationДокумент27 страницAntibody Identificationhamaada100% (1)
- Antibody DetectionДокумент7 страницAntibody DetectionhamaadaОценок пока нет
- ABO Reversing TestДокумент2 страницыABO Reversing TesthamaadaОценок пока нет
- Ab IdentificationДокумент4 страницыAb IdentificationhamaadaОценок пока нет
- Antibody DetectionДокумент7 страницAntibody DetectionhamaadaОценок пока нет
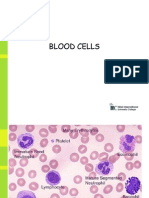
- Blood CellsДокумент7 страницBlood CellshamaadaОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- ABO Forward TestingДокумент2 страницыABO Forward TestinghamaadaОценок пока нет
- Blood Group SystemsДокумент7 страницBlood Group SystemshamaadaОценок пока нет
- Haemolytic AnaemiaДокумент11 страницHaemolytic AnaemiahamaadaОценок пока нет
- Blood Collection & ProcessingДокумент29 страницBlood Collection & ProcessinghamaadaОценок пока нет
- ABO Grouping ProcedureДокумент2 страницыABO Grouping ProcedurehamaadaОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Abo Blood GroupДокумент26 страницAbo Blood GrouphamaadaОценок пока нет
- Virgilio S. Delima V. Susan Mercaida Gois GR NO. 178352 - June 17, 2008 FactsДокумент6 страницVirgilio S. Delima V. Susan Mercaida Gois GR NO. 178352 - June 17, 2008 FactsNikki BarenaОценок пока нет
- Department of Education: Republic of The PhilippinesДокумент3 страницыDepartment of Education: Republic of The PhilippinesAdonis BesaОценок пока нет
- AssemblyinstructionsДокумент12 страницAssemblyinstructionsPriscila AzevedoОценок пока нет
- Telangana Budget 2014-2015 Full TextДокумент28 страницTelangana Budget 2014-2015 Full TextRavi Krishna MettaОценок пока нет
- Frequency Meter by C Programming of AVR MicrocontrДокумент3 страницыFrequency Meter by C Programming of AVR MicrocontrRajesh DhavaleОценок пока нет
- JWCh06 PDFДокумент23 страницыJWCh06 PDF007featherОценок пока нет
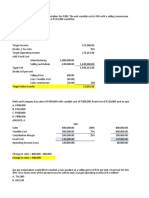
- CVP Solution (Quiz)Документ9 страницCVP Solution (Quiz)Angela Miles DizonОценок пока нет
- CLC Customer Info Update Form v3Документ1 страницаCLC Customer Info Update Form v3John Philip Repol LoberianoОценок пока нет
- Etp ListДокумент33 страницыEtp ListMohamed MostafaОценок пока нет
- 2023 Prospectus 2Документ69 страниц2023 Prospectus 2miclau1123Оценок пока нет
- KL Wellness City LIvewell 360 2023Документ32 страницыKL Wellness City LIvewell 360 2023tan sietingОценок пока нет
- Central BankДокумент65 страницCentral BankFarazNaseer100% (1)
- Using The Marketing Mix Reading Comprenhension TaskДокумент17 страницUsing The Marketing Mix Reading Comprenhension TaskMonica GalvisОценок пока нет
- Mint Delhi 13-12-2022Документ18 страницMint Delhi 13-12-2022Ayush sethОценок пока нет
- Programming in Java Assignment 8: NPTEL Online Certification Courses Indian Institute of Technology KharagpurДокумент4 страницыProgramming in Java Assignment 8: NPTEL Online Certification Courses Indian Institute of Technology KharagpurPawan NaniОценок пока нет
- Ielts Band 9 Sample Essay NoДокумент5 страницIelts Band 9 Sample Essay NoNhã NguyễnОценок пока нет
- DEFCON ManualДокумент13 страницDEFCON Manualbuyvalve100% (1)
- Determining Total Impulse and Specific Impulse From Static Test DataДокумент4 страницыDetermining Total Impulse and Specific Impulse From Static Test Datajai_selvaОценок пока нет
- Chapter 1 - Introduction To Computer NetworksДокумент32 страницыChapter 1 - Introduction To Computer NetworksHuluОценок пока нет
- Company's Profile Presentation (Mauritius Commercial Bank)Документ23 страницыCompany's Profile Presentation (Mauritius Commercial Bank)ashairways100% (2)
- Job Hazard Analysis TemplateДокумент2 страницыJob Hazard Analysis TemplateIzmeer JaslanОценок пока нет
- Funded African Tech Startups 2020Документ13 страницFunded African Tech Startups 2020LoОценок пока нет
- Fleck 3150 Downflow: Service ManualДокумент40 страницFleck 3150 Downflow: Service ManualLund2016Оценок пока нет
- Converting An XML File With Many Hierarchy Levels To ABAP FormatДокумент8 страницConverting An XML File With Many Hierarchy Levels To ABAP FormatGisele Cristina Betencourt de OliveiraОценок пока нет
- Bid Document PDFДокумент125 страницBid Document PDFAzharudin ZoechnyОценок пока нет
- Enhancing reliability of CRA piping welds with PAUTДокумент10 страницEnhancing reliability of CRA piping welds with PAUTMohsin IamОценок пока нет
- Risk Ology ManualДокумент2 страницыRisk Ology ManualGregoryОценок пока нет
- Racial and Ethnic Challenges in the UAE vs UKДокумент16 страницRacial and Ethnic Challenges in the UAE vs UKATUL KORIОценок пока нет
- Current Affairs Q&A PDF June 9 2023 by Affairscloud 1Документ21 страницаCurrent Affairs Q&A PDF June 9 2023 by Affairscloud 1Yashika GuptaОценок пока нет
- Duty Entitlement Pass BookДокумент3 страницыDuty Entitlement Pass BookSunail HussainОценок пока нет