Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Azevedo Slum English 1926Документ90 страницAzevedo Slum English 1926Nealon Isaacs100% (1)
- Marcato Capital - Letter To Lifetime Fitness BoardДокумент13 страницMarcato Capital - Letter To Lifetime Fitness BoardCanadianValueОценок пока нет
- IHL 1 BALLB ProjectДокумент16 страницIHL 1 BALLB Projectabcde fghikjОценок пока нет
- Compiler Design MCQ Question Bank Last Update 29-Dec-20202 Page 1 of 18Документ18 страницCompiler Design MCQ Question Bank Last Update 29-Dec-20202 Page 1 of 18SOMENATH ROY CHOUDHURYОценок пока нет
- Distosia BahuДокумент185 страницDistosia BahuAdith Fileanugraha100% (1)
- Performance AnalyticsДокумент193 страницыPerformance AnalyticsGОценок пока нет
- 1st Year Unit 7 Writing A Letter About A CelebrationДокумент2 страницы1st Year Unit 7 Writing A Letter About A CelebrationmlooooolОценок пока нет
- Youcastr Case StudyДокумент2 страницыYoucastr Case StudyMomina NadeemОценок пока нет
- TracheostomyДокумент6 страницTracheostomynamithaОценок пока нет
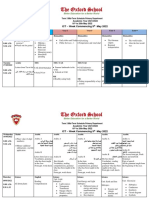
- Term 3 Mid-Term Assessment ScheduleДокумент9 страницTerm 3 Mid-Term Assessment ScheduleRabia MoeedОценок пока нет
- CatalysisДокумент50 страницCatalysisnagendra_rdОценок пока нет
- Bareilly Ki Barfi Full Movie DownloadДокумент3 страницыBareilly Ki Barfi Full Movie Downloadjobair100% (3)
- Competition Commission of India: Mahendra SoniДокумент16 страницCompetition Commission of India: Mahendra SoniSuman sharmaОценок пока нет
- Health COX's Monthly Dashboard - 2023 NovДокумент4 страницыHealth COX's Monthly Dashboard - 2023 Novcox mamОценок пока нет
- Fc406 q1 Tabilin, GizelleДокумент3 страницыFc406 q1 Tabilin, GizelleGizelle Alcantara-TabilinОценок пока нет
- Ptfe ManufacturingДокумент16 страницPtfe ManufacturingKokki Kumar Dpce100% (1)
- LESSON 1 Overview of Toeic Speaking WritingДокумент29 страницLESSON 1 Overview of Toeic Speaking WritingPhạm Thị HuyềnОценок пока нет
- How Is The Frog's Stomach Adapted To Provide An Increased Digestive Surface?Документ6 страницHow Is The Frog's Stomach Adapted To Provide An Increased Digestive Surface?Jemuel Bucud LagartoОценок пока нет
- Perceived Impact of Community Policing On Crime Prevention and Public Safety in Ozamiz CityДокумент7 страницPerceived Impact of Community Policing On Crime Prevention and Public Safety in Ozamiz Cityjabezgaming02Оценок пока нет
- Consent For MTP PDFДокумент4 страницыConsent For MTP PDFMajid SheikhОценок пока нет
- Fugacity and Fugacity CoeffДокумент9 страницFugacity and Fugacity CoeffMujtabba AlkhtatОценок пока нет
- (Cambridge Studies in Opera) Victoria Johnson, Jane F. Fulcher, Thomas Ertman-Opera and Society in Italy and France From Monteverdi To Bourdieu-Cambridge University Press (2007) PDFДокумент440 страниц(Cambridge Studies in Opera) Victoria Johnson, Jane F. Fulcher, Thomas Ertman-Opera and Society in Italy and France From Monteverdi To Bourdieu-Cambridge University Press (2007) PDFnbozekidis100% (3)
- Bob Trish Duggan FoundationДокумент19 страницBob Trish Duggan FoundationWilfried HandlОценок пока нет
- Brand Relevance - 1Документ2 страницыBrand Relevance - 1Ayan PandaОценок пока нет
- History of English Culture and Literature MidДокумент4 страницыHistory of English Culture and Literature Midfirdasalsa59Оценок пока нет
- Intersection of Psychology With Architecture Final ReportДокумент22 страницыIntersection of Psychology With Architecture Final Reportmrunmayee pandeОценок пока нет
- 000 Digital Control LecturesДокумент67 страниц000 Digital Control LecturesPX PRОценок пока нет
- Subject: Managerial Accounting Topic: Total Quality Management Reporter: Romalyn R. PurificacionДокумент2 страницыSubject: Managerial Accounting Topic: Total Quality Management Reporter: Romalyn R. Purificacionromalyn purificacionОценок пока нет
- Translator Resume SampleДокумент2 страницыTranslator Resume SampleIsabel JimenezОценок пока нет
- Gripped by The Mystery: Franziska Carolina Rehbein SspsДокумент70 страницGripped by The Mystery: Franziska Carolina Rehbein SspsdonteldontelОценок пока нет