Вам также может понравиться
- Word Catheter PlacementДокумент3 страницыWord Catheter PlacementTiara AnggrainiОценок пока нет
- MedSurg RecitДокумент3 страницыMedSurg RecitnicoleОценок пока нет
- Drainage Through Periodontal Pocket.: Acute AbscessДокумент2 страницыDrainage Through Periodontal Pocket.: Acute AbscessShirmayne TangОценок пока нет
- Bartholin's Cyst/AbscessДокумент6 страницBartholin's Cyst/AbscessJane NathaniaОценок пока нет
- Case Study 2Документ7 страницCase Study 2desdav100% (1)
- Unified HC Protocols For Minor SurgeriesДокумент4 страницыUnified HC Protocols For Minor Surgeriesrv bombetaОценок пока нет
- Standard Measures of Management of Infected WoundДокумент11 страницStandard Measures of Management of Infected WoundMohamed FarahatОценок пока нет
- Abdominal ParacentesisДокумент5 страницAbdominal ParacentesisVijith.V.kumar100% (1)
- Incision & Drainage of Abscess Group 9 4bДокумент5 страницIncision & Drainage of Abscess Group 9 4bGUDISELA ramyaОценок пока нет
- BiopsyДокумент24 страницыBiopsyOsamaОценок пока нет
- Procedures in O&GДокумент7 страницProcedures in O&GAbdulrahman NajiОценок пока нет
- Incision and Drainage Procedure - UpToDate PDFДокумент1 страницаIncision and Drainage Procedure - UpToDate PDFLeslieОценок пока нет
- Case Study Main OtДокумент56 страницCase Study Main Otamier_s100% (1)
- Bartholin'S Cyst and Abscess: North Dakota Family Planning Program Protocols - Reproductive DiseasesДокумент2 страницыBartholin'S Cyst and Abscess: North Dakota Family Planning Program Protocols - Reproductive DiseasesMilanisti22Оценок пока нет
- Ostomy CareДокумент3 страницыOstomy CareSyamsul ArifinОценок пока нет
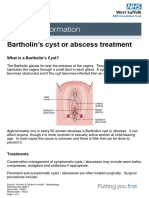
- Bartholin's Cyst or Abscess TreatmentДокумент4 страницыBartholin's Cyst or Abscess TreatmentRezaFArthaОценок пока нет
- 12 - Oral BiopsyДокумент11 страниц12 - Oral BiopsyMahmoud TayseerОценок пока нет
- Colostomy CareДокумент6 страницColostomy CareLoren Sales ReyesОценок пока нет
- Scaling and Root PlaningДокумент12 страницScaling and Root Planingbasel alogily100% (1)
- Incision and Drainage of AbscessesДокумент25 страницIncision and Drainage of Abscessesjaphetnwapi100% (1)
- ACUTE Wound ManagementДокумент9 страницACUTE Wound Managementelisabeth hutaurukОценок пока нет
- NCP LeukemiaДокумент5 страницNCP LeukemiaTriciaОценок пока нет
- Bone Marrow AspirationДокумент6 страницBone Marrow AspirationSai PardhuОценок пока нет
- Bites and ManagementДокумент4 страницыBites and ManagementSrishti KhullarОценок пока нет
- Patient Education Sheet For Warts TreatmentДокумент7 страницPatient Education Sheet For Warts TreatmentHalim MaherОценок пока нет
- Tubes and Drains: Foley CatheterДокумент9 страницTubes and Drains: Foley CatheterWesam Al-TawilОценок пока нет
- Vesico Vaginal FistulaДокумент6 страницVesico Vaginal Fistulaapi-3705046Оценок пока нет
- Sajo College of Nursing Sciences Birnin Kebbi, Kebbi State: Unit IxДокумент22 страницыSajo College of Nursing Sciences Birnin Kebbi, Kebbi State: Unit IxyusufОценок пока нет
- BTK Quick Hits FinalДокумент19 страницBTK Quick Hits FinalMujahed LaswiОценок пока нет
- BTK Quick Hits Final PDFДокумент24 страницыBTK Quick Hits Final PDFcusom34Оценок пока нет
- Pre and OpДокумент6 страницPre and OpFatimah Alshareef100% (1)
- Impaired Skin IntegДокумент2 страницыImpaired Skin IntegMarcus Philip GonzalesОценок пока нет
- Reproductive - Genital System-2Документ26 страницReproductive - Genital System-2Muhammad Faheem AslamОценок пока нет
- 13) Safety DrillsДокумент7 страниц13) Safety DrillsJAYR GABIANAОценок пока нет
- 6 Urinary EliminationДокумент5 страниц6 Urinary EliminationkhautedameОценок пока нет
- Rafols, Janna Mae L. 3F-2C OR QuestionsДокумент8 страницRafols, Janna Mae L. 3F-2C OR QuestionsJan Crizza Dale R. FrancoОценок пока нет
- 2003 EXAM PrintedДокумент12 страниц2003 EXAM PrintedZarin Khan100% (2)
- Nov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Документ79 страницNov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Jean Gwyneth GatchalianОценок пока нет
- Basic Principles in Management of Patients With Maxillofacial InjuriesДокумент11 страницBasic Principles in Management of Patients With Maxillofacial InjuriesVishnu S PattathОценок пока нет
- Snake Bites MainДокумент6 страницSnake Bites MainElvisОценок пока нет
- Dilatation and Curettage ProcedureДокумент3 страницыDilatation and Curettage Proceduresagi muОценок пока нет
- Blood Urea Nitrogen (BUN) : Posted: 05 Sep 2010 10:11 PM PDTДокумент9 страницBlood Urea Nitrogen (BUN) : Posted: 05 Sep 2010 10:11 PM PDTLanie Reyes de GuzmanОценок пока нет
- Principles of Tissue Biopsy in Oral and MaxillofacialДокумент34 страницыPrinciples of Tissue Biopsy in Oral and MaxillofacialEdmond Apriza DrgОценок пока нет
- Nursing Diagnosis For TonsillitisДокумент3 страницыNursing Diagnosis For TonsillitisVaneca Go67% (9)
- Intrevenous TherapyДокумент5 страницIntrevenous TherapyCharles DoradoОценок пока нет
- COLOSTOMYДокумент5 страницCOLOSTOMYZhyraine Iraj D. CaluzaОценок пока нет
- ColostomyДокумент5 страницColostomyZhyraine Iraj D. Caluza100% (1)
- Skin Sutures and StaplesДокумент4 страницыSkin Sutures and StaplesDrmirfat AlkashifОценок пока нет
- Esophageal Perforation TreatmentДокумент4 страницыEsophageal Perforation TreatmentDabessa MosissaОценок пока нет
- Presentation DEEPTHIДокумент17 страницPresentation DEEPTHIsarathchandran deepthiОценок пока нет
- 2003 ExamДокумент10 страниц2003 ExamBibek Raj100% (1)
- Paracentesis 040641Документ10 страницParacentesis 040641Mike Faustino SolangonОценок пока нет
- Radiation TherapyДокумент2 страницыRadiation TherapyAngel Joy CatalanОценок пока нет
- Management of Facial LacerationДокумент2 страницыManagement of Facial LacerationAssist Professor Dr-Bayad Jaza MahmudОценок пока нет
- SOPs To Deliver Safe Paediatric CareДокумент11 страницSOPs To Deliver Safe Paediatric Carearadhya asthanaОценок пока нет
- Abdominal Injuries Last FormДокумент25 страницAbdominal Injuries Last FormOmar MohammedОценок пока нет
- Journal AbssДокумент5 страницJournal AbssMilanisti22Оценок пока нет
- Bartholin Cyst or Abscess v2 Apr 14 PDFДокумент2 страницыBartholin Cyst or Abscess v2 Apr 14 PDFTeguh Imana NugrahaОценок пока нет
- Different in the therapy of pressure negtotheeva single-useОт EverandDifferent in the therapy of pressure negtotheeva single-useОценок пока нет
- Opini-Can Hemoglobin-Hematocrit Relationship Be Used To Assess Hydration StatusДокумент4 страницыOpini-Can Hemoglobin-Hematocrit Relationship Be Used To Assess Hydration StatusBoby ShéОценок пока нет
- 10 Fascinating Facts About SurgeryДокумент11 страниц10 Fascinating Facts About SurgeryArlynn Lontoc De RamosОценок пока нет
- Treatment FluorosisДокумент3 страницыTreatment Fluorosisdr parveen bathlaОценок пока нет
- Five Methods of Breast Volume Measurement: A Comparative Study of Measurements of Specimen Volume in 30 Mastectomy CasesДокумент10 страницFive Methods of Breast Volume Measurement: A Comparative Study of Measurements of Specimen Volume in 30 Mastectomy CasesDIOGENESОценок пока нет
- Neonatal ResuscitationДокумент15 страницNeonatal ResuscitationAmruta GadeОценок пока нет
- Med Ethics CasesДокумент17 страницMed Ethics CasesBernard Fernandez100% (1)
- Quality Survey QuestionnaireДокумент13 страницQuality Survey QuestionnaireDeepak KaushikОценок пока нет
- CPTДокумент2 страницыCPTmmaitehmdОценок пока нет
- Haraprasanna Das GuptaДокумент312 страницHaraprasanna Das Guptamikembad100% (2)
- ABORTIONДокумент23 страницыABORTIONCristyl Shine BariaoОценок пока нет
- Soal Un UnsratДокумент80 страницSoal Un UnsratSuzetteОценок пока нет
- E HEALTH SeminarДокумент17 страницE HEALTH SeminarDev jibreenОценок пока нет
- Phillips HD3 Operators ManualДокумент322 страницыPhillips HD3 Operators Manualdave78% (9)
- Noorani 2014Документ3 страницыNoorani 2014MD Luthfy LubisОценок пока нет
- Women Factory Employees Facilities As Per Factory ActДокумент25 страницWomen Factory Employees Facilities As Per Factory ActNaveen Kumar SharmaОценок пока нет
- Manual of Clinical DieteticsДокумент7 страницManual of Clinical Dieteticsandi agung0% (1)
- Midwifery Pharmacology-9Документ1 страницаMidwifery Pharmacology-9georgeloto12Оценок пока нет
- Ijphrd Journal July-Sep 2013 - 06-06-213 PDFДокумент307 страницIjphrd Journal July-Sep 2013 - 06-06-213 PDFp1843dОценок пока нет
- 300 BededДокумент13 страниц300 BededSamta Soni83% (6)
- Historical Review of MidwiferyДокумент32 страницыHistorical Review of MidwiferyVinayak SrivastavaОценок пока нет
- General Surgery: Dr. S. Gallinge R Gord On Bud Uhan and Sam Minor, e D Itors Dana M Kay, Associate e D ItorДокумент56 страницGeneral Surgery: Dr. S. Gallinge R Gord On Bud Uhan and Sam Minor, e D Itors Dana M Kay, Associate e D ItorKamran AfzalОценок пока нет
- Non-Emergency Patient Transport: What Are The Quality and Safety Issues? A Systematic ReviewДокумент8 страницNon-Emergency Patient Transport: What Are The Quality and Safety Issues? A Systematic Reviewmahadabrata21Оценок пока нет
- Untitled - Susan BlumДокумент65 страницUntitled - Susan BlumnewОценок пока нет
- 1.anatomy of The PleuraДокумент17 страниц1.anatomy of The PleuraMangayakkarasi Telukanam0% (1)
- Carefusion-Monitors and AnalyzersДокумент9 страницCarefusion-Monitors and Analyzersrubenr25Оценок пока нет
- 4 Steps: Instrument PassingДокумент3 страницы4 Steps: Instrument PassingGwyn Leen CagasОценок пока нет
- Pedo Tooth AnomaliesДокумент5 страницPedo Tooth Anomalieszuperzilch1676Оценок пока нет
- Health Teaching Plan To A Mother in A Pre-Natal SettingДокумент8 страницHealth Teaching Plan To A Mother in A Pre-Natal SettingChris GuisadioОценок пока нет
- Intrapartum Fetal Monitoring: R. EUGENE BAILEY, MD, SUNY Upstate Medical University, Syracuse, New YorkДокумент9 страницIntrapartum Fetal Monitoring: R. EUGENE BAILEY, MD, SUNY Upstate Medical University, Syracuse, New YorkOana CristinaОценок пока нет
- Comparison of Intermittent Bolus and Continuous Infusion Techniques For Administration of Atracurium in Renal FailureДокумент5 страницComparison of Intermittent Bolus and Continuous Infusion Techniques For Administration of Atracurium in Renal FailureWantoSKepОценок пока нет