Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- NBME 22 OfflineДокумент200 страницNBME 22 OfflineGautham Kanagala86% (14)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Torc 4 Abscohort1 - CompressДокумент13 страницTorc 4 Abscohort1 - CompressFaye MartinezОценок пока нет
- Appointment Letter Staff Nurse Job DescriptionДокумент3 страницыAppointment Letter Staff Nurse Job DescriptionRenita ChrisОценок пока нет
- Personality TestДокумент5 страницPersonality Testapi-215089876Оценок пока нет
- F.E. Campbell - Sweet Slavery - HIT 139Документ115 страницF.E. Campbell - Sweet Slavery - HIT 139HokusLocus67% (3)
- Healthy Voice: by Dan VascДокумент22 страницыHealthy Voice: by Dan VascscoutjohnyОценок пока нет
- Foreign Bodies in The Ear, Nose, and Throat: Steven W. Heim, MD, MSPH, and Karen L. Maughan, MDДокумент5 страницForeign Bodies in The Ear, Nose, and Throat: Steven W. Heim, MD, MSPH, and Karen L. Maughan, MDWidya SusilowatiОценок пока нет
- Set Fess and MaksilofasialДокумент21 страницаSet Fess and MaksilofasialFranspolОценок пока нет
- Gambar Basic Set FessДокумент12 страницGambar Basic Set FessFranspolОценок пока нет
- Pentatonic ScaleДокумент1 страницаPentatonic ScaleFranspolОценок пока нет
- 20071217030304.noise Induced Hearing Loss PresentationДокумент22 страницы20071217030304.noise Induced Hearing Loss PresentationmawarmelatiОценок пока нет
- Bells PalsyДокумент63 страницыBells PalsyBunga DewanggiОценок пока нет
- Behrbohm HДокумент1 страницаBehrbohm HFranspolОценок пока нет
- Foreign Bodies in The Ear, Nose, and Throat: Steven W. Heim, MD, MSPH, and Karen L. Maughan, MDДокумент5 страницForeign Bodies in The Ear, Nose, and Throat: Steven W. Heim, MD, MSPH, and Karen L. Maughan, MDWidya SusilowatiОценок пока нет
- 04 Diphtheria7pДокумент21 страница04 Diphtheria7pSaravan PramodОценок пока нет
- Basic Ear Anatomy GuideДокумент23 страницыBasic Ear Anatomy GuideFranspolОценок пока нет
- NystagmusДокумент4 страницыNystagmusFranspolОценок пока нет
- Aminoglycoside OtotoxicityДокумент6 страницAminoglycoside OtotoxicityFranspolОценок пока нет
- Pentatonic ScaleДокумент1 страницаPentatonic ScaleFranspolОценок пока нет
- Daftar PustkaДокумент2 страницыDaftar PustkaFranspolОценок пока нет
- Behrbohm H, Et Al. 2009. Mouth and Phrynx. Ear, Nose, and Throat Diseases: With Head and Neck Surgery, P 268Документ1 страницаBehrbohm H, Et Al. 2009. Mouth and Phrynx. Ear, Nose, and Throat Diseases: With Head and Neck Surgery, P 268FranspolОценок пока нет
- AHD - Neuro-Opthalmology - V. Patel - NYSTAGMUSДокумент22 страницыAHD - Neuro-Opthalmology - V. Patel - NYSTAGMUSFranspolОценок пока нет
- DifteriДокумент7 страницDifteriFranspolОценок пока нет
- Papi Llo Matos IsДокумент10 страницPapi Llo Matos IsFranspolОценок пока нет
- ECG InterpretationДокумент52 страницыECG InterpretationFranspol50% (2)
- Dependence of The Middle EarДокумент6 страницDependence of The Middle EarFranspolОценок пока нет
- Acute MastoiditisДокумент6 страницAcute MastoiditisFranspolОценок пока нет
- Recurrent Respiratory Papillomatosis (RRP) : Basic Science To Clinical StudiesДокумент16 страницRecurrent Respiratory Papillomatosis (RRP) : Basic Science To Clinical StudiesLaura PayneОценок пока нет
- AHD - Neuro-Opthalmology - V. Patel - NYSTAGMUSДокумент22 страницыAHD - Neuro-Opthalmology - V. Patel - NYSTAGMUSFranspolОценок пока нет
- Football Manager 2011Документ2 страницыFootball Manager 2011FranspolОценок пока нет
- ImmunotherapyДокумент11 страницImmunotherapyFranspolОценок пока нет
- A Case of Acquired Tracheal Diverticulum Presenting With Globus PharyngeusДокумент3 страницыA Case of Acquired Tracheal Diverticulum Presenting With Globus PharyngeusFranspolОценок пока нет
- Progressive Hearing Loss Following Acquired Cytomegalovirus Infection in An Immunocompromised ChildДокумент4 страницыProgressive Hearing Loss Following Acquired Cytomegalovirus Infection in An Immunocompromised ChildFranspolОценок пока нет
- Wheat Sourdough Fermentation - Effects of Time and Acidification On Fundamental Rheological PropertiesДокумент9 страницWheat Sourdough Fermentation - Effects of Time and Acidification On Fundamental Rheological PropertiesmaurodiloretoОценок пока нет
- Zollinger-Ellison Syndrome (Gastrinoma)Документ15 страницZollinger-Ellison Syndrome (Gastrinoma)Huy QuangОценок пока нет
- PackageCare Maintenance ChecklistДокумент1 страницаPackageCare Maintenance ChecklistBùi ViệtОценок пока нет
- Rocket Motor Head-end Structural AnalysisДокумент83 страницыRocket Motor Head-end Structural AnalysisRudra Sai SandeepОценок пока нет
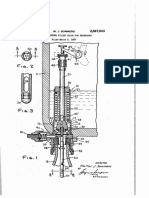
- Counter-pressure filler valve for beveragesДокумент3 страницыCounter-pressure filler valve for beveragesbimalishaОценок пока нет
- Manoshe Street Takeaway MenuДокумент9 страницManoshe Street Takeaway MenuimaddakrОценок пока нет
- WCDMA Optimization Case StudyДокумент60 страницWCDMA Optimization Case StudyRamesh Nikam100% (1)
- Nursing Care of The Patient Undergoing Lumbar Spinal Fusion: ReviewsДокумент10 страницNursing Care of The Patient Undergoing Lumbar Spinal Fusion: ReviewsMuammar100% (1)
- Public Health EngineeringДокумент10 страницPublic Health EngineeringOmkar DeshpandeОценок пока нет
- Girl Scouts ActivitiesДокумент5 страницGirl Scouts ActivitiessluttybitchОценок пока нет
- What Do You Already Know?: True TrueДокумент3 страницыWhat Do You Already Know?: True TrueJeffrey MangaoangОценок пока нет
- Trilon C Types TI enДокумент11 страницTrilon C Types TI enjuanfelipehincapieОценок пока нет
- Glover 6e - Chapter 02Документ41 страницаGlover 6e - Chapter 02JIGNESH DESAIОценок пока нет
- Accessibility POC: October 26, 2017Документ7 страницAccessibility POC: October 26, 2017Ramesh BodukaniОценок пока нет
- Flashcards - CP4 Preparation of A Standard Solution and Titration - Edexcel IAL Chemistry A-LevelДокумент37 страницFlashcards - CP4 Preparation of A Standard Solution and Titration - Edexcel IAL Chemistry A-LevelTravel UnlimitedОценок пока нет
- Aire Acondicionado Mazda 3 2006Документ2 страницыAire Acondicionado Mazda 3 2006Jhon ConnorОценок пока нет
- EWC661 TITLE: Dietary Habits During Term Time Among University Students. Background of StudyДокумент4 страницыEWC661 TITLE: Dietary Habits During Term Time Among University Students. Background of StudyfarinaazmiОценок пока нет
- Roof Construction Dr. Fixit Newcoat PDFДокумент1 страницаRoof Construction Dr. Fixit Newcoat PDFRishabh VijayОценок пока нет
- Physics Investigatory Project Class 12Документ12 страницPhysics Investigatory Project Class 12shivanginirai7Оценок пока нет
- How Game-Based Teaching Strategy Affect The Student's Learning in MathematicsДокумент13 страницHow Game-Based Teaching Strategy Affect The Student's Learning in MathematicsAaron Jay BulataoОценок пока нет
- LV CB Catalogue PDFДокумент260 страницLV CB Catalogue PDFBoobesh Kumar SekarОценок пока нет
- Shandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23Документ130 страницShandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23mliugong94% (16)
- SECTION 03380 Post-Tensioned Concrete Rev 1Документ30 страницSECTION 03380 Post-Tensioned Concrete Rev 1Abdalrahman AntariОценок пока нет
- Envl 4300 Lab3Документ9 страницEnvl 4300 Lab3api-662867343Оценок пока нет
- Case 1Документ25 страницCase 1hamshiniОценок пока нет