Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- +the Origins and Nature of Compassion Focused Therapy.Документ37 страниц+the Origins and Nature of Compassion Focused Therapy.juaromerОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Karp, Sociological Communitarianism and The Just CommunityДокумент21 страницаKarp, Sociological Communitarianism and The Just CommunityjuaromerОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Libro Enfoques PDFДокумент262 страницыLibro Enfoques PDFAna Rivera CastañonОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- +2017 Auditory Verbal Hallucinations and The Differential Diagnosis of Schizophrenia and Dissociative DisordersДокумент10 страниц+2017 Auditory Verbal Hallucinations and The Differential Diagnosis of Schizophrenia and Dissociative DisordersjuaromerОценок пока нет
- 2017 - Behavioral AddictionsДокумент6 страниц2017 - Behavioral AddictionsjuaromerОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- ++ On The Seductions of Psychoanalytic Story-Telling - Narcissism and The Problems of NarrativeДокумент18 страниц++ On The Seductions of Psychoanalytic Story-Telling - Narcissism and The Problems of NarrativejuaromerОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- ++L. Mark S. Micale, Paul Lerner-Traumatic Pasts - History, Psychiatry, and Trauma in The Modern Age, 1870-1930-Cambridge University Press (2001)Документ333 страницы++L. Mark S. Micale, Paul Lerner-Traumatic Pasts - History, Psychiatry, and Trauma in The Modern Age, 1870-1930-Cambridge University Press (2001)juaromer50% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Conklin Malone Fowler 2012 Mentalization and The RorschachДокумент26 страницConklin Malone Fowler 2012 Mentalization and The RorschachjuaromerОценок пока нет
- The Contribution of Forensic Psycodiagnostic in Legal Medical Evaluations Regarding The Amendment of Sex Assignment The Rorschach Test 2157 7145 1000276Документ5 страницThe Contribution of Forensic Psycodiagnostic in Legal Medical Evaluations Regarding The Amendment of Sex Assignment The Rorschach Test 2157 7145 1000276juaromerОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- ++how Is Poverty Transmitted IntergenerationallyДокумент40 страниц++how Is Poverty Transmitted IntergenerationallyjuaromerОценок пока нет
- The Significance of The Rorschach Pure Color ResponseДокумент6 страницThe Significance of The Rorschach Pure Color ResponsejuaromerОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- ++2016 Review, Psychological Testing That Matters, Creating A Road Map For Effective TreatmentДокумент5 страниц++2016 Review, Psychological Testing That Matters, Creating A Road Map For Effective TreatmentjuaromerОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Pai 2004 Performance of Personality Assessment Inventory andДокумент4 страницыPai 2004 Performance of Personality Assessment Inventory andjuaromerОценок пока нет
- Convergent and Incremental Validity of The MMPI-2 and Rorschach On Psychotic-Related PDFДокумент107 страницConvergent and Incremental Validity of The MMPI-2 and Rorschach On Psychotic-Related PDFjuaromerОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- 2015, Standards, Accuracy, and Questions of Bias in Rorschach Meta-AnalysesДокумент11 страниц2015, Standards, Accuracy, and Questions of Bias in Rorschach Meta-AnalysesjuaromerОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Psychological Characteristics of Japanese Patients Chornic Pain PDFДокумент13 страницPsychological Characteristics of Japanese Patients Chornic Pain PDFjuaromerОценок пока нет
- 2010 The Measurement of Social Competence PDFДокумент12 страниц2010 The Measurement of Social Competence PDFjuaromerОценок пока нет
- 1992, Meloy, Revisiting The Rorschach of Sirhan SirhanДокумент23 страницы1992, Meloy, Revisiting The Rorschach of Sirhan SirhanjuaromerОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- 2012, Laimou, An Epistemological and Methodological Approach To Drives and DiffusionДокумент17 страниц2012, Laimou, An Epistemological and Methodological Approach To Drives and DiffusionjuaromerОценок пока нет
- Gronnerod - Rorschach Assessment of Changes After PsychotherДокумент21 страницаGronnerod - Rorschach Assessment of Changes After PsychotherjuaromerОценок пока нет
- Normative Study of Rorschach (Parisian School) For Brazilian AdolescentДокумент10 страницNormative Study of Rorschach (Parisian School) For Brazilian AdolescentjuaromerОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- 2015, Standards, Accuracy, and Questions of Bias in Rorschach Meta-AnalysesДокумент11 страниц2015, Standards, Accuracy, and Questions of Bias in Rorschach Meta-AnalysesjuaromerОценок пока нет
- Burlay Lazzari Content BorderДокумент8 страницBurlay Lazzari Content BorderjuaromerОценок пока нет
- The Use of The Rorschach Comprehensive System As An Assessment of Depression in AdolesДокумент169 страницThe Use of The Rorschach Comprehensive System As An Assessment of Depression in AdolesjuaromerОценок пока нет
- Convergent and Incremental Validity of The MMPI-2 and Rorschach On Psychotic-Related PDFДокумент107 страницConvergent and Incremental Validity of The MMPI-2 and Rorschach On Psychotic-Related PDFjuaromerОценок пока нет
- The Use of The Rorschach Comprehensive System As An Assessment of Depression in AdolesДокумент169 страницThe Use of The Rorschach Comprehensive System As An Assessment of Depression in AdolesjuaromerОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- ++introduction To The Special Section On Multicultural and Community. Clinical Psychology in ContextДокумент3 страницы++introduction To The Special Section On Multicultural and Community. Clinical Psychology in ContextjuaromerОценок пока нет
- 2013 Rorschach Measures of Cognition Relate To Everyday and Social Functioning ViglioneДокумент11 страниц2013 Rorschach Measures of Cognition Relate To Everyday and Social Functioning ViglionejuaromerОценок пока нет
- A Philosophy of Clinical SupervisionДокумент13 страницA Philosophy of Clinical SupervisionNick Judson100% (1)
- Rabinovich Rorschach Personality Correlates of ElectroencephaloДокумент13 страницRabinovich Rorschach Personality Correlates of ElectroencephalojuaromerОценок пока нет
- Job Description-EA To MDДокумент2 страницыJob Description-EA To MDamartyaray2003Оценок пока нет
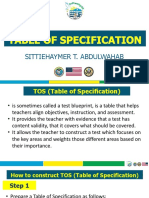
- Sittiehaymer T. AbdulwahabДокумент17 страницSittiehaymer T. AbdulwahabHymerОценок пока нет
- Numerology The Complete Guide Vol-2 TextДокумент373 страницыNumerology The Complete Guide Vol-2 TextMadalina100% (1)
- Research ProposalДокумент17 страницResearch Proposaladiti dhoteОценок пока нет
- Options To Anger For The Phoenix Program PDFДокумент206 страницOptions To Anger For The Phoenix Program PDFBon Ha GuОценок пока нет
- Liya Xuan Push Hands 35 PointsДокумент11 страницLiya Xuan Push Hands 35 PointsKen TwchongОценок пока нет
- Two Conceptions of Vacuum SedleyДокумент20 страницTwo Conceptions of Vacuum SedleylicenciaturafilosofiaunilaОценок пока нет
- NoticeДокумент9 страницNoticeeuniceОценок пока нет
- Prepare Second Edition Level 1: Unit 2 Grammar: PlusДокумент2 страницыPrepare Second Edition Level 1: Unit 2 Grammar: PlusCarola RojasОценок пока нет
- Self LoveДокумент19 страницSelf LoveRian Kusuma Dewi100% (2)
- Perpetual Succour Academy, Inc.: National RD., Poblacion Dos, Malabuyoc, CebuДокумент4 страницыPerpetual Succour Academy, Inc.: National RD., Poblacion Dos, Malabuyoc, CebuKen FerrolinoОценок пока нет
- 2016 PCE Exam Policy English 150812 v3Документ32 страницы2016 PCE Exam Policy English 150812 v3Sam100% (1)
- The Effects of Social IsolationДокумент13 страницThe Effects of Social IsolationGlady Joy Manalo MellaОценок пока нет
- Cross-Cultural Differences in The Effects of Abstract and Concrete Thinking On Imagery Generation and Ad Persuasion PDFДокумент35 страницCross-Cultural Differences in The Effects of Abstract and Concrete Thinking On Imagery Generation and Ad Persuasion PDFViolaQianОценок пока нет
- Item AnalysisДокумент16 страницItem AnalysisFil IlaganОценок пока нет
- Chapter 1 and 2 Slides From Research Methods For Business by Uma SekaranДокумент23 страницыChapter 1 and 2 Slides From Research Methods For Business by Uma SekaranALi Raza KhanОценок пока нет
- Set Yourself Up For Presentation Success WorksheetДокумент3 страницыSet Yourself Up For Presentation Success WorksheetAhmad Ibrahim Makki MarufОценок пока нет
- The Problem and It'S SettingДокумент32 страницыThe Problem and It'S SettingMara PundavelaОценок пока нет
- Gadeers ResumeДокумент1 страницаGadeers Resumeapi-396563097Оценок пока нет
- Delhi University MA English Entrance Previous Year Question Paper 2019 PDFДокумент38 страницDelhi University MA English Entrance Previous Year Question Paper 2019 PDFSayari DebbarmaОценок пока нет
- Hubungan Antara Aktivitas Fisik Dengan Kelelahan Kerja Pada Tenaga Kerja Bongkar MuatДокумент6 страницHubungan Antara Aktivitas Fisik Dengan Kelelahan Kerja Pada Tenaga Kerja Bongkar Muatlusia dirahОценок пока нет
- 30 15 Short Interval 1.5 PDFДокумент8 страниц30 15 Short Interval 1.5 PDFBLLYDОценок пока нет
- Chapter 009Документ18 страницChapter 009HannaОценок пока нет
- Archangel ArielДокумент5 страницArchangel ArielRamanОценок пока нет
- InsightДокумент15 страницInsightjitendraОценок пока нет
- Applying Choices and PossibilitiesДокумент3 страницыApplying Choices and PossibilitiesSpeech & Language Therapy in PracticeОценок пока нет
- HIDALGO COUNTY - Edinburg ISD - 2000 Texas School Survey of Drug and Alcohol UseДокумент10 страницHIDALGO COUNTY - Edinburg ISD - 2000 Texas School Survey of Drug and Alcohol UseTexas School Survey of Drug and Alcohol UseОценок пока нет
- Grovo HigherEd Microlearning Whitepaper PDFДокумент17 страницGrovo HigherEd Microlearning Whitepaper PDFchoopo100% (1)
- BDPДокумент23 страницыBDPShivendu AnandОценок пока нет
- Notes in Pe 12#1Документ3 страницыNotes in Pe 12#1Kersey Badocdoc100% (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryОт EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryРейтинг: 4.5 из 5 звезд4.5/5 (157)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionОт EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionОценок пока нет