Вам также может понравиться
- Galatians Chapter 5 Translation 1-15 1Документ3 страницыGalatians Chapter 5 Translation 1-15 1JohnОценок пока нет
- Lecture Notes On GalatiansДокумент8 страницLecture Notes On GalatiansJohnОценок пока нет
- Galatians Chapter 5.16-25 Translation 16Документ3 страницыGalatians Chapter 5.16-25 Translation 16JohnОценок пока нет
- Biblical Hermeneutics EssayДокумент13 страницBiblical Hermeneutics EssayJohnОценок пока нет
- Opening Lecture HermeneuticsДокумент5 страницOpening Lecture HermeneuticsJohnОценок пока нет
- Barth Vs BrunnerДокумент3 страницыBarth Vs BrunnerJohnОценок пока нет
- Trinity Lecture 4Документ5 страницTrinity Lecture 4JohnОценок пока нет
- The Aftermath of War in EuropeДокумент2 страницыThe Aftermath of War in EuropeJohnОценок пока нет
- Themes in Kings and ChroniclesДокумент1 страницаThemes in Kings and ChroniclesJohnОценок пока нет
- Of Justification and The Justification of God and NT Wright's, JustificationДокумент3 страницыOf Justification and The Justification of God and NT Wright's, JustificationJohnОценок пока нет
- Dissertation HandoutДокумент1 страницаDissertation HandoutJohnОценок пока нет
- Contextual: 26 As Compared To The TraditionalДокумент13 страницContextual: 26 As Compared To The TraditionalJohnОценок пока нет
- Value Vision Ethos Mexico CityДокумент3 страницыValue Vision Ethos Mexico CityJohnОценок пока нет
- The Tale of Two Moravian Missionaries: Ten Shekels and A ShirtДокумент1 страницаThe Tale of Two Moravian Missionaries: Ten Shekels and A ShirtJohn100% (1)
- Ed., Chichester: Wiley-Blackwell, 2010, 189Документ6 страницEd., Chichester: Wiley-Blackwell, 2010, 189JohnОценок пока нет
- Christology EssayДокумент6 страницChristology EssayJohnОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Samsung CL21K3W PDFДокумент4 страницыSamsung CL21K3W PDFNelson Muñoz BautistaОценок пока нет
- Lecture 1 - Surveying FieldworkДокумент16 страницLecture 1 - Surveying FieldworkArchitect ArchitectОценок пока нет
- A New Four-Scroll Chaotic System With A Self-Excited Attractor and Circuit ImplementationДокумент5 страницA New Four-Scroll Chaotic System With A Self-Excited Attractor and Circuit ImplementationMada Sanjaya WsОценок пока нет
- Deloitte IT Governance SurveyДокумент20 страницDeloitte IT Governance Surveymrehan2k2Оценок пока нет
- Disconnected ManДокумент4 страницыDisconnected ManBecky100% (1)
- Evermotion Archmodels Vol 40 PDFДокумент2 страницыEvermotion Archmodels Vol 40 PDFJustinОценок пока нет
- 2690 2 2023 PDFДокумент12 страниц2690 2 2023 PDFDevesh Kumar PandeyОценок пока нет
- Arrays in C++Документ13 страницArrays in C++weggie alcarazОценок пока нет
- The Essential Guide To Developing A Social Recruiting StrategyДокумент48 страницThe Essential Guide To Developing A Social Recruiting Strategysubzzz222Оценок пока нет
- Mechanistic-Empirical Pavement Design GuideДокумент3 страницыMechanistic-Empirical Pavement Design Guidelelu8210Оценок пока нет
- High School Kids Science Fiction Short StoriesДокумент5 страницHigh School Kids Science Fiction Short StoriesHarshal bhardwaj100% (1)
- Return To Tranquility Ven - PunnajiДокумент109 страницReturn To Tranquility Ven - PunnajiNorah GravelleОценок пока нет
- Vessel Nozzle PDFДокумент30 страницVessel Nozzle PDFEugenia LorenzaОценок пока нет
- Ibt TOEFL Reading-IsuДокумент10 страницIbt TOEFL Reading-IsuShinОценок пока нет
- Zero Based BudgetingДокумент2 страницыZero Based BudgetingVincentcius Pratama WahyuОценок пока нет
- Proposit Gen MathДокумент9 страницProposit Gen MathAngelika AndresОценок пока нет
- Karpagam College of EngineeringДокумент6 страницKarpagam College of EngineeringSuresh VpОценок пока нет
- Redshift C4D Material Pack 3 Helpful TipsДокумент21 страницаRedshift C4D Material Pack 3 Helpful TipsDreck FresseОценок пока нет
- 09 04 2016-Online-ExamДокумент46 страниц09 04 2016-Online-ExamAtharva Sheersh PandeyОценок пока нет
- Aavit 5 AДокумент113 страницAavit 5 AAnonymous ok5UankОценок пока нет
- Family Day by Day - The Guide To A Successful Family LifeДокумент212 страницFamily Day by Day - The Guide To A Successful Family Lifeprajya100% (3)
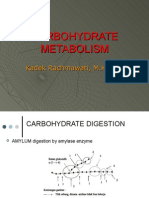
- Carbohydrate MetabolismДокумент38 страницCarbohydrate Metabolismwidya nurrohmanОценок пока нет
- Carol Jones: Res Publica 8: 295-299, 2002Документ6 страницCarol Jones: Res Publica 8: 295-299, 2002Colton McKeeОценок пока нет
- Exadata Technical Whitepaper 134575Документ31 страницаExadata Technical Whitepaper 134575Jyothi JohnОценок пока нет
- Creating The Fusion EconomyДокумент15 страницCreating The Fusion Economyrocket_science3.0Оценок пока нет
- Vibration MeasurementДокумент20 страницVibration MeasurementDae A VeritasОценок пока нет
- 169-Article Text-987-1-10-20220530Документ8 страниц169-Article Text-987-1-10-20220530Ika PratiwiОценок пока нет
- Ex 5308-Alexandra Thedeby-Heating and Cooling With Solar Powered Peltier ElementsДокумент93 страницыEx 5308-Alexandra Thedeby-Heating and Cooling With Solar Powered Peltier ElementsMohammad NaufalОценок пока нет
- Alternative ADHD TreatmentДокумент3 страницыAlternative ADHD TreatmentCindy VanegasОценок пока нет
- Dario Great Wall of China Lesson PlanДокумент3 страницыDario Great Wall of China Lesson Planapi-297914033Оценок пока нет