Вам также может понравиться
- Jump Stretch November 2014Документ2 страницыJump Stretch November 2014jmfleckОценок пока нет
- BCRC Dec 2014 ScheduleДокумент16 страницBCRC Dec 2014 SchedulejmfleckОценок пока нет
- Jump Stretch November 2014Документ2 страницыJump Stretch November 2014jmfleckОценок пока нет
- Cycling & Hot Yoga Nov 2014 CalendarДокумент1 страницаCycling & Hot Yoga Nov 2014 CalendarjmfleckОценок пока нет
- August 2014 ScheduleДокумент16 страницAugust 2014 SchedulejmfleckОценок пока нет
- Pool ScheduleДокумент1 страницаPool SchedulejmfleckОценок пока нет
- 2014-2015 Dance Class RegistrationДокумент1 страница2014-2015 Dance Class RegistrationjmfleckОценок пока нет
- Nov 2014 ScheduleДокумент8 страницNov 2014 SchedulejmfleckОценок пока нет
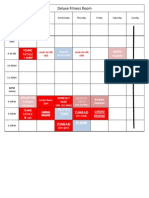
- Deluxe Fitness Nov 2014 CalendarДокумент1 страницаDeluxe Fitness Nov 2014 CalendarjmfleckОценок пока нет
- Youth Gymnastics Class Schedule 2014-2015: Class Ages DAY TimeДокумент1 страницаYouth Gymnastics Class Schedule 2014-2015: Class Ages DAY TimejmfleckОценок пока нет
- 5K FormДокумент2 страницы5K FormjmfleckОценок пока нет
- TriFold - 5KДокумент2 страницыTriFold - 5KjmfleckОценок пока нет
- 2014-2015 Dance ClassДокумент1 страница2014-2015 Dance ClassjmfleckОценок пока нет
- Expo 2014 FormДокумент1 страницаExpo 2014 FormjmfleckОценок пока нет
- Gymnastics Registration Payment Due 2013-2014Документ1 страницаGymnastics Registration Payment Due 2013-2014jmfleckОценок пока нет
- Jump Stretch August 2014Документ2 страницыJump Stretch August 2014jmfleckОценок пока нет
- Intake FormДокумент1 страницаIntake FormjmfleckОценок пока нет
- Deluxe Fitness BrochuresДокумент2 страницыDeluxe Fitness BrochuresjmfleckОценок пока нет
- Gymnastics Registration 2014Документ1 страницаGymnastics Registration 2014jmfleckОценок пока нет
- Pre School CampДокумент1 страницаPre School CampjmfleckОценок пока нет
- July 2014 ScheduleДокумент12 страницJuly 2014 SchedulejmfleckОценок пока нет
- All Questions, Contact: Michelle Bower (724) 699-4383: 2014-2015 Dance ScheduleДокумент1 страницаAll Questions, Contact: Michelle Bower (724) 699-4383: 2014-2015 Dance SchedulejmfleckОценок пока нет
- Best of The BestДокумент1 страницаBest of The BestjmfleckОценок пока нет
- 1st Annual Golf Scramble BrochureДокумент2 страницы1st Annual Golf Scramble BrochurejmfleckОценок пока нет
- 401 - Northern Route To Downtown Sharon (Monday-Friday)Документ9 страниц401 - Northern Route To Downtown Sharon (Monday-Friday)jmfleckОценок пока нет
- Racquetball TournamentДокумент1 страницаRacquetball TournamentjmfleckОценок пока нет
- J Marcus FleckДокумент1 страницаJ Marcus FleckjmfleckОценок пока нет
- Wish ListДокумент3 страницыWish ListjmfleckОценок пока нет
- HistoryДокумент1 страницаHistoryjmfleckОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Filipino Value System and Its Effects On BusinessДокумент4 страницыThe Filipino Value System and Its Effects On BusinessQueleОценок пока нет
- Consulting ProcessДокумент42 страницыConsulting Processmyfragilehart1992100% (2)
- Portfolio SociolinguisticsДокумент7 страницPortfolio SociolinguisticsAndreea-Raluca ManeaОценок пока нет
- PR 2Документ30 страницPR 2Jan Lymar BecteОценок пока нет
- Shoe Dog - Phil Knight: Different of The Men of His AgeДокумент4 страницыShoe Dog - Phil Knight: Different of The Men of His Agescribdbugmenot1919Оценок пока нет
- Understanding English 2 Budget and LessonsДокумент11 страницUnderstanding English 2 Budget and LessonsAnnaliza GalangОценок пока нет
- Twin Flame Healing With Feminine Power 21 Day Practice PDFДокумент37 страницTwin Flame Healing With Feminine Power 21 Day Practice PDFmargaritosa100% (5)
- HIVE AcknowledgmentДокумент9 страницHIVE AcknowledgmentKim CiudadanoОценок пока нет
- Drama JourneyДокумент24 страницыDrama JourneyMJ FoustОценок пока нет
- Celebrity Worship SyndromeДокумент21 страницаCelebrity Worship SyndromeVictoria JungОценок пока нет
- Autohipnosis UltradianaДокумент32 страницыAutohipnosis UltradianaOespiritodedeus MestreОценок пока нет
- BSC Case Study Telecom FijiДокумент35 страницBSC Case Study Telecom Fijiiuliamaria18Оценок пока нет
- BAFI507 M&A Course OverviewДокумент10 страницBAFI507 M&A Course Overviewuygh g100% (1)
- DepEd's Commitment to InclusionДокумент39 страницDepEd's Commitment to InclusionCamille AguilarОценок пока нет
- Consumer Behaviour InterviewДокумент1 страницаConsumer Behaviour Interviewnirosha niroshaОценок пока нет
- Orlando Patterson - Slavery and Social Death - A Comparative StudyДокумент265 страницOrlando Patterson - Slavery and Social Death - A Comparative Studymccss100% (8)
- LISTENING Test 1 - 1Документ3 страницыLISTENING Test 1 - 1Aitor Alonso LanzaОценок пока нет
- A Resource-baseTdhe Ory of The Firm: Knowledge Versus OpportunismДокумент26 страницA Resource-baseTdhe Ory of The Firm: Knowledge Versus Opportunismxaxif8265Оценок пока нет
- Initial Data Base For Family Nursing PracticeДокумент12 страницInitial Data Base For Family Nursing Practicemiss RN67% (18)
- Merit Badge Counselor ApplicationДокумент2 страницыMerit Badge Counselor ApplicationRussell NashОценок пока нет
- TCC Quiz SpiДокумент3 страницыTCC Quiz SpiGilbert Gabrillo JoyosaОценок пока нет
- Marketing Notes For SBI Clerk ExamДокумент5 страницMarketing Notes For SBI Clerk ExamGirija VaniОценок пока нет
- Milestone05 Mwega Nkanda 11.06.2023Документ13 страницMilestone05 Mwega Nkanda 11.06.2023ConradОценок пока нет
- What Color Sounds Like IbaДокумент7 страницWhat Color Sounds Like Ibaapi-279311830Оценок пока нет
- Nietzsche On Truth and LiesДокумент8 страницNietzsche On Truth and LiesCristian AlinОценок пока нет
- Cancer Support GroupДокумент13 страницCancer Support GroupIndah PratiwiОценок пока нет
- Telling Our Stories, Sharing Our Lives: A Collection of Student Memoir WritingДокумент133 страницыTelling Our Stories, Sharing Our Lives: A Collection of Student Memoir WritingbrayanОценок пока нет
- Leadership and Nursing Care Management 5th Edition Huber Test BankДокумент26 страницLeadership and Nursing Care Management 5th Edition Huber Test BankSharonSheppardnpby100% (48)
- Moving Up Guest Speaker Message EnglishДокумент2 страницыMoving Up Guest Speaker Message EnglishClarence CarreonОценок пока нет
- Family Therapy Working With Challenging Family Dynamics in Effective MannerДокумент76 страницFamily Therapy Working With Challenging Family Dynamics in Effective MannerManishaОценок пока нет