Вам также может понравиться
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Class12cbsechemistrypracticals 150123140020 Conversion Gate01Документ26 страницClass12cbsechemistrypracticals 150123140020 Conversion Gate01Stephen Anthony WijayaОценок пока нет
- TnO Teaching PreДокумент2 страницыTnO Teaching PreStephen Anthony WijayaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Catachol Oxidase Practical As BioДокумент1 страницаCatachol Oxidase Practical As BioStephen Anthony WijayaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Biology Practical 3Документ3 страницыBiology Practical 3Stephen Anthony WijayaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Calculating The Respiratory QuotientДокумент1 страницаCalculating The Respiratory QuotientStephen Anthony WijayaОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- ChemistryДокумент23 страницыChemistrychicarito786Оценок пока нет
- Chemistry Revision Notes Ch.2Документ5 страницChemistry Revision Notes Ch.2Stephen Anthony WijayaОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Advocacy LetterДокумент2 страницыAdvocacy Letterapi-236671577Оценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Achievements of UAE UnionДокумент11 страницAchievements of UAE UnionShahroz Asif100% (5)
- Medi-Cal Choice Form: Highly ConfidentialДокумент2 страницыMedi-Cal Choice Form: Highly Confidentialxk05Оценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- Pancha Karma (Sree Subramania Ayurvedic Nursing Home)Документ15 страницPancha Karma (Sree Subramania Ayurvedic Nursing Home)Sanand Ratnam Thekkayil100% (1)
- EBPДокумент1 страницаEBPShreyas WalvekarОценок пока нет
- Chapter 25 InformaticsДокумент76 страницChapter 25 InformaticsJa DimasОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Chapter 8: Health Systems ResponsivenessДокумент26 страницChapter 8: Health Systems Responsivenessshashi hegdeОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Eye Med SummaryДокумент2 страницыEye Med SummaryparthaОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Value Based HealthcareДокумент48 страницValue Based HealthcareAsem Shadid100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Pharmaceutical Benefits Under State Medical Assistance Programs, 2000Документ583 страницыPharmaceutical Benefits Under State Medical Assistance Programs, 2000National Pharmaceutical Council100% (3)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- HEADLINE: Health Economics 101 BYLINE: by Paul Krugman Bob Herbert Is On Vacation. BodyДокумент8 страницHEADLINE: Health Economics 101 BYLINE: by Paul Krugman Bob Herbert Is On Vacation. BodyJohn_Lee_8554Оценок пока нет
- Stainless Steel Crowns SSC-Primary and Permanent: Shan Lal, Dds Director, Pre-Clinical Programs Pediatric DentistryДокумент4 страницыStainless Steel Crowns SSC-Primary and Permanent: Shan Lal, Dds Director, Pre-Clinical Programs Pediatric DentistryfradmardОценок пока нет
- Latest Payment Details for OFWДокумент1 страницаLatest Payment Details for OFWDan William BadiqueОценок пока нет
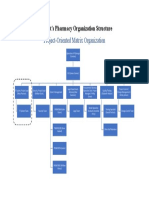
- Wilmont Organization Structure-Wilmont's PharmacyДокумент1 страницаWilmont Organization Structure-Wilmont's PharmacySalah Ud DinОценок пока нет
- ICD-10 Planning GuideДокумент4 страницыICD-10 Planning GuideObat Dot In100% (1)
- Evidence Based Critical CareДокумент6 страницEvidence Based Critical CareSreetamSahaОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Requirements for Validating Medical CertificatesДокумент2 страницыRequirements for Validating Medical CertificatesAlvin Xtian NucumОценок пока нет
- Carriere® SLX Patient EducationДокумент2 страницыCarriere® SLX Patient EducationOrtho OrganizersОценок пока нет
- IM Presentation-PRICING STRATEGY (Revised)Документ33 страницыIM Presentation-PRICING STRATEGY (Revised)palakОценок пока нет
- Health Advocate's StoryДокумент4 страницыHealth Advocate's StoryHealth Advocate, Inc.Оценок пока нет
- LMC ICD-10 PowerPointДокумент77 страницLMC ICD-10 PowerPointNicholas HenryОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Healthcare SPSSДокумент6 страницHealthcare SPSSvdragicaОценок пока нет
- Healthcare CFO Operations Leader in Indianapolis IN Resume William Kevin FowlerДокумент3 страницыHealthcare CFO Operations Leader in Indianapolis IN Resume William Kevin FowlerWilliamKevinFowlerОценок пока нет
- Arcalling 49 Denial Scenarios - Medical Billing Ar Calling JobsДокумент39 страницArcalling 49 Denial Scenarios - Medical Billing Ar Calling JobsJagadeesh SuraОценок пока нет
- SOP FinalДокумент7 страницSOP FinalsabaОценок пока нет
- HDFC Network Hospital List - June'23Документ868 страницHDFC Network Hospital List - June'23SanОценок пока нет
- Narayana Hrudalaya's strategic health insurance offeringДокумент4 страницыNarayana Hrudalaya's strategic health insurance offeringPrateek100% (1)
- IDN & GPO in USAДокумент2 страницыIDN & GPO in USAreddykmpОценок пока нет
- SAIL CSR Project Report GroupДокумент18 страницSAIL CSR Project Report GroupSumeet DubeyОценок пока нет
- Sunil Healthcare Consultant 5yr Exp PDFДокумент4 страницыSunil Healthcare Consultant 5yr Exp PDFsunilroutОценок пока нет