Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- NCM 106 SyllabusДокумент3 страницыNCM 106 Syllabusguevarraannette100% (8)
- SQL ServerДокумент30 страницSQL Serverjimmy_sam001Оценок пока нет
- TPF 4 Work Plan and Methodology 02-12-15 (Final) ANDREДокумент30 страницTPF 4 Work Plan and Methodology 02-12-15 (Final) ANDREAndrea BroccoliОценок пока нет
- Sports - Safety and First Aid CGДокумент5 страницSports - Safety and First Aid CGJonel CatanguiОценок пока нет
- HAAD ReviewerДокумент35 страницHAAD ReviewerSydRey92% (24)
- LAFD Field ManualДокумент122 страницыLAFD Field Manualfumptfxn50% (4)
- Triage: Hospital Emergency Awareness and Response TrainingДокумент34 страницыTriage: Hospital Emergency Awareness and Response TrainingrgiemorenoОценок пока нет
- TriageДокумент40 страницTriagemody94546Оценок пока нет
- Midterm Quiz - NCM 106.2016Документ4 страницыMidterm Quiz - NCM 106.2016Andrea BroccoliОценок пока нет
- JCI HandbookДокумент88 страницJCI Handbookamirali.bme452767% (6)
- 4 TH Ed CHK ListДокумент70 страниц4 TH Ed CHK ListArpita mishraОценок пока нет
- ATLS Notes PDFДокумент46 страницATLS Notes PDFTilly Mandal100% (3)
- SOP EMERGENCY and Vehicular Accident 2017Документ60 страницSOP EMERGENCY and Vehicular Accident 2017Ramona FlowersОценок пока нет
- NCM 118 and 119 All Notes For ProcessingДокумент38 страницNCM 118 and 119 All Notes For ProcessingBern NerquitОценок пока нет
- Community Health Nursing: Practice of Nursing in Local/national Health DepartmentsДокумент6 страницCommunity Health Nursing: Practice of Nursing in Local/national Health DepartmentsAndrea BroccoliОценок пока нет
- Jci Tool 7th Edition - HN VersionДокумент380 страницJci Tool 7th Edition - HN Versionactive66100% (4)
- Natural Disasters and Their Global ImpactДокумент17 страницNatural Disasters and Their Global ImpactgandhialpitОценок пока нет
- BSN II Comprehensive Examination 2nd Sem 2017Документ12 страницBSN II Comprehensive Examination 2nd Sem 2017Andrea Broccoli100% (1)
- Disaster NursingДокумент5 страницDisaster NursingLorelie Asis100% (1)
- CHN & CD Pre-Board TestДокумент6 страницCHN & CD Pre-Board TestAndrea Broccoli100% (1)
- Nurse Assesses Client with Appendicitis and Increased PainДокумент28 страницNurse Assesses Client with Appendicitis and Increased PainAndrea BroccoliОценок пока нет
- Comprehension, vocabulary, grammar and customer service exercisesДокумент3 страницыComprehension, vocabulary, grammar and customer service exercisesAndrea Broccoli100% (1)
- Community Health Nursing Compre.2015with RatioДокумент8 страницCommunity Health Nursing Compre.2015with RatioAndrea BroccoliОценок пока нет
- André Gil Sabanal: Education SkillsДокумент1 страницаAndré Gil Sabanal: Education SkillsAndrea BroccoliОценок пока нет
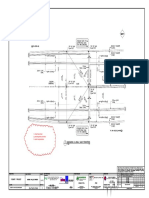
- Location Outfall To Nula Tula - of 1 2 3 4 5Документ1 страницаLocation Outfall To Nula Tula - of 1 2 3 4 5Andrea BroccoliОценок пока нет
- CDDJ Vol03 Iss1 2 PDFДокумент10 страницCDDJ Vol03 Iss1 2 PDFAndrea BroccoliОценок пока нет
- CDDJ Vol03 Iss1 2 PDFДокумент10 страницCDDJ Vol03 Iss1 2 PDFAndrea BroccoliОценок пока нет
- CDDJ Vol03 Iss1 2 PDFДокумент10 страницCDDJ Vol03 Iss1 2 PDFAndrea BroccoliОценок пока нет
- HEC2 CommentДокумент4 страницыHEC2 CommentAndrea BroccoliОценок пока нет
- For Structural Engineer To Check/comment: The MRT 7 ProjectДокумент1 страницаFor Structural Engineer To Check/comment: The MRT 7 ProjectAndrea BroccoliОценок пока нет
- Field Inspection ReportДокумент10 страницField Inspection ReportAndrea BroccoliОценок пока нет
- 1, Show Flow Arrows 2. Provide Profile and Levels 3. Submit Computations 'Документ2 страницы1, Show Flow Arrows 2. Provide Profile and Levels 3. Submit Computations 'Andrea BroccoliОценок пока нет
- RW-3A HD: 2000 RW-3B HD: 2001 - 3000: The MRT 7 ProjectДокумент2 страницыRW-3A HD: 2000 RW-3B HD: 2001 - 3000: The MRT 7 ProjectAndrea BroccoliОценок пока нет
- Minutes of The MeetingДокумент1 страницаMinutes of The MeetingAndrea BroccoliОценок пока нет
- F DoredДокумент1 страницаF DoredAndrea BroccoliОценок пока нет
- Not SummarizedДокумент22 страницыNot SummarizedAndrea BroccoliОценок пока нет
- Field Inspection ReportДокумент10 страницField Inspection ReportAndrea BroccoliОценок пока нет
- FDC Billing DavaoДокумент2 страницыFDC Billing DavaoAndrea BroccoliОценок пока нет
- NCM 106.cardioДокумент2 страницыNCM 106.cardioAndrea BroccoliОценок пока нет
- Introductio N To Informatic S: Lectur e 7: Modelin G TH e Worl DДокумент13 страницIntroductio N To Informatic S: Lectur e 7: Modelin G TH e Worl DAndrea BroccoliОценок пока нет
- Exam 1-50Документ4 страницыExam 1-50Andrea BroccoliОценок пока нет
- Introductio N To Informatic S: Lectur e 6: Histor y of Compute Rs (Par T II)Документ23 страницыIntroductio N To Informatic S: Lectur e 6: Histor y of Compute Rs (Par T II)Andrea BroccoliОценок пока нет
- TPF 5 - Key Staff For IC Mactan 02-12-15 (Final) ANDREДокумент6 страницTPF 5 - Key Staff For IC Mactan 02-12-15 (Final) ANDREAndrea BroccoliОценок пока нет
- Safety Officer CV: Andre Gil SabanalДокумент9 страницSafety Officer CV: Andre Gil SabanalAndrea BroccoliОценок пока нет
- Tactical Emergency Medical Support (Tems) Course Overview and Instructional GoalsДокумент11 страницTactical Emergency Medical Support (Tems) Course Overview and Instructional GoalsAnonymous pOggsIhOMОценок пока нет
- NCP AccДокумент19 страницNCP AccAthyrah KadirОценок пока нет
- Chapter 2 Casualty AssessmentДокумент32 страницыChapter 2 Casualty AssessmentAnna MethyldaОценок пока нет
- Assessment of Knowledge and Skills of Triage AmongДокумент6 страницAssessment of Knowledge and Skills of Triage AmongKivilcim Cinar OkuslugОценок пока нет
- Medical Surgical Nursing Lecture I MonthlyДокумент9 страницMedical Surgical Nursing Lecture I MonthlyJohn Lyndon SayongОценок пока нет
- Etat Module Kenya For Distance LearnersДокумент242 страницыEtat Module Kenya For Distance Learnersokwadha simion100% (1)
- Emergency Department ExplainedДокумент10 страницEmergency Department ExplainedramneekОценок пока нет
- ECHO Indicators AnalysisДокумент3 страницыECHO Indicators AnalysisNgoma TélesphoreОценок пока нет
- Philippines Health Facility Self-Assessment Form COVID-19 IPCДокумент9 страницPhilippines Health Facility Self-Assessment Form COVID-19 IPCquesterОценок пока нет
- A Proposed Model For Outpatient Care Service Improvement Using The Healthcare Lean Approach and SimulationДокумент6 страницA Proposed Model For Outpatient Care Service Improvement Using The Healthcare Lean Approach and SimulationGuillermo Luis AcostaОценок пока нет
- 16.0 Emergency Unit: DescriptionДокумент18 страниц16.0 Emergency Unit: DescriptionMudita PiseОценок пока нет
- 24-Hour-Triage Acute OncologyДокумент16 страниц24-Hour-Triage Acute OncologySilviu MorteanuОценок пока нет
- Educational Competencies For Registered Nurses (MCIs)Документ15 страницEducational Competencies For Registered Nurses (MCIs)jasnate84100% (1)
- Disaster ManagementДокумент42 страницыDisaster ManagementLoma Waghmare (Jadhav)Оценок пока нет
- Otas (Notwg)Документ10 страницOtas (Notwg)Fransiscus Braveno RapaОценок пока нет
- The Important Role of Nurses in Disaster ResponseДокумент8 страницThe Important Role of Nurses in Disaster ResponsejnetОценок пока нет