Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Biological Warfare Agents - AgronДокумент129 страницBiological Warfare Agents - AgronMARK ARQUE LACANARIAОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Multigrade Lesson Plan in English3Документ13 страницMultigrade Lesson Plan in English3Nick Bantolo100% (11)
- Lecture 7 Dystocia in Farm AnimalsДокумент39 страницLecture 7 Dystocia in Farm AnimalsgnpobsОценок пока нет
- Krause S Food The Nutrition Care Process PDFДокумент3 страницыKrause S Food The Nutrition Care Process PDFAndrei Oanes18% (11)
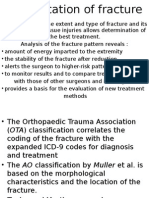
- Classification of FracturesДокумент9 страницClassification of FracturesazkaparobiОценок пока нет
- Villena 2004Документ4 страницыVillena 2004azkaparobiОценок пока нет
- Kompetensi ObgynДокумент1 страницаKompetensi ObgynazkaparobiОценок пока нет
- Weight ChumleaДокумент5 страницWeight ChumleaazkaparobiОценок пока нет
- Nutritional Assessment of Elderly Persons in Babylon: Hadeel Fadhil FarhoodДокумент8 страницNutritional Assessment of Elderly Persons in Babylon: Hadeel Fadhil FarhoodazkaparobiОценок пока нет
- 6 Respectful Baby Sleep Solutions Freebie 21fe39a1 A163 4d22 b5f2 9d5261e10772Документ4 страницы6 Respectful Baby Sleep Solutions Freebie 21fe39a1 A163 4d22 b5f2 9d5261e10772Jamie AsuncionОценок пока нет
- Community Nursing ProcessДокумент10 страницCommunity Nursing Processbuhari rabiuОценок пока нет
- Renal Drug StudyДокумент3 страницыRenal Drug StudyRiva OlarteОценок пока нет
- Food Power For AthletesДокумент3 страницыFood Power For AthletesVegan Future100% (1)
- Physical Education Cambridge Progression Test P1 - ST6 (2022)Документ14 страницPhysical Education Cambridge Progression Test P1 - ST6 (2022)Givemore MuromboОценок пока нет
- 03 Irum Tazeb InsuДокумент3 страницы03 Irum Tazeb InsuNimra MalikОценок пока нет
- Glossary & Introduction. 4 EditionДокумент7 страницGlossary & Introduction. 4 EditionSilviu MorteanuОценок пока нет
- hw499 Unit 9 Resume Assignment Stacey Story FinalДокумент3 страницыhw499 Unit 9 Resume Assignment Stacey Story Finalapi-651674228Оценок пока нет
- A Novel Clinical Grading Scale To Guide The Management of Crusted ScabiesДокумент6 страницA Novel Clinical Grading Scale To Guide The Management of Crusted ScabiesFelisiana KasmanОценок пока нет
- InvaginasiДокумент10 страницInvaginasimelchiadiОценок пока нет
- Pyromania-The Urge To Set Fires For Pleasure, Gratification, or Release of Tension Ezhae SymptomsДокумент2 страницыPyromania-The Urge To Set Fires For Pleasure, Gratification, or Release of Tension Ezhae SymptomsptbarnabicОценок пока нет
- Public Health in Community Settings: An IntroductionДокумент22 страницыPublic Health in Community Settings: An IntroductionRusevОценок пока нет
- Final ResearchДокумент65 страницFinal ResearchHarbrinder GurmОценок пока нет
- Lesson1Introductionanddigestion 211227 100329Документ7 страницLesson1Introductionanddigestion 211227 100329Chavi SvsОценок пока нет
- Segurança e Tax de Lesoes PDFДокумент20 страницSegurança e Tax de Lesoes PDFFilipeAssunçãoОценок пока нет
- Epidemiology Course For 3 Yrs Midwifery Students: Yibekal .M (PHA, PH and MPH/Specialty Epidemiology)Документ326 страницEpidemiology Course For 3 Yrs Midwifery Students: Yibekal .M (PHA, PH and MPH/Specialty Epidemiology)Yoseph KassaОценок пока нет
- Soal PAS BIG Xi, SMT 3, OnlineДокумент10 страницSoal PAS BIG Xi, SMT 3, OnlineRivaldi Lukman HakimОценок пока нет
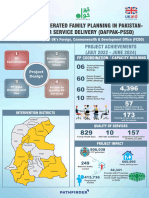
- Poster Sindh 2-01-2024Документ11 страницPoster Sindh 2-01-2024FM Printers111Оценок пока нет
- Nebulization ProcedureДокумент4 страницыNebulization ProcedureDhan IvanОценок пока нет
- Contoh FMEA UIHC Burn Unit Patient Education DocumentationДокумент2 страницыContoh FMEA UIHC Burn Unit Patient Education DocumentationAnisaОценок пока нет
- Consolidated Guidelines OnДокумент594 страницыConsolidated Guidelines OnRICHARD EDUARDO FERNANDEZ SAENZОценок пока нет
- Disaster Nursing Lecture 1Документ11 страницDisaster Nursing Lecture 1Beahtriz GuintoОценок пока нет
- Babe 2Документ17 страницBabe 2Sathish SizzyОценок пока нет
- Azithromycin For Acute Exacerbations of Asthma The AZALEA Randomized Clinical TrialДокумент8 страницAzithromycin For Acute Exacerbations of Asthma The AZALEA Randomized Clinical TrialicaeeeОценок пока нет
- Meperidine Hydro ChlorideДокумент4 страницыMeperidine Hydro Chlorideapi-3797941Оценок пока нет
- Site167 26375 en File1Документ11 страницSite167 26375 en File1Cao Minh TríОценок пока нет