Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Satisfaction Attributes and Satisfaction of Customers: The Case of Korean Restaurants in BataanДокумент10 страницSatisfaction Attributes and Satisfaction of Customers: The Case of Korean Restaurants in BataanMaraОценок пока нет
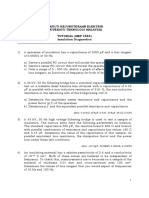
- Tutorial MEP1553 - Insulation DiagnosticsДокумент4 страницыTutorial MEP1553 - Insulation DiagnosticsSharin Bin Ab GhaniОценок пока нет
- NMIMS Offer LetterДокумент4 страницыNMIMS Offer LetterSUBHAJITОценок пока нет
- Among Us Hack Mod Menu Mod AlwaysДокумент4 страницыAmong Us Hack Mod Menu Mod AlwaysC JОценок пока нет
- 29!541 Transient Aspects of Unloading Oil and Gas Wells With Coiled TubingДокумент6 страниц29!541 Transient Aspects of Unloading Oil and Gas Wells With Coiled TubingWaode GabriellaОценок пока нет
- Io TДокумент2 страницыIo TPrasanth VarasalaОценок пока нет
- List of TCP and UDP Port NumbersДокумент44 страницыList of TCP and UDP Port NumbersElvis JavierОценок пока нет
- Instruction Manual Series 880 CIU Plus: July 2009 Part No.: 4416.526 Rev. 6Документ44 страницыInstruction Manual Series 880 CIU Plus: July 2009 Part No.: 4416.526 Rev. 6nknico100% (1)
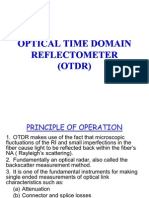
- OTDRДокумент57 страницOTDRarijeetdguy3051100% (1)
- ELEN 325 Lab 1 PrelabДокумент8 страницELEN 325 Lab 1 PrelabAndrew ZellerОценок пока нет
- UNV EZAccess Datasheet - V1.2-EN - 883121 - 168459 - 0Документ3 страницыUNV EZAccess Datasheet - V1.2-EN - 883121 - 168459 - 0Agus NetОценок пока нет
- Bank Reconciliation and Proof of CashДокумент2 страницыBank Reconciliation and Proof of CashDarwyn HonaОценок пока нет
- Pipenet: A Wireless Sensor Network For Pipeline MonitoringДокумент11 страницPipenet: A Wireless Sensor Network For Pipeline MonitoringMykola YarynovskyiОценок пока нет
- What Is Aggregate DemandqwertДокумент9 страницWhat Is Aggregate DemandqwertShahana KhanОценок пока нет
- 02 Adaptive Tracking Control of A Nonholonomic Mobile RobotДокумент7 страниц02 Adaptive Tracking Control of A Nonholonomic Mobile Robotchoc_ngoayОценок пока нет
- Dy DX: NPTEL Course Developer For Fluid Mechanics Dr. Niranjan Sahoo Module 04 Lecture 33 IIT-GuwahatiДокумент7 страницDy DX: NPTEL Course Developer For Fluid Mechanics Dr. Niranjan Sahoo Module 04 Lecture 33 IIT-GuwahatilawanОценок пока нет
- Implementation of BS 8500 2006 Concrete Minimum Cover PDFДокумент13 страницImplementation of BS 8500 2006 Concrete Minimum Cover PDFJimmy Lopez100% (1)
- MEETING 12 - Additional CasesДокумент25 страницMEETING 12 - Additional CasesJohn Michael VidaОценок пока нет
- Manual de Colisión Mazda 626 1986-1987Документ9 страницManual de Colisión Mazda 626 1986-1987mark rueОценок пока нет
- Material DevOps Essentials DEPC enДокумент88 страницMaterial DevOps Essentials DEPC enCharlineОценок пока нет
- PBR ImplementationДокумент32 страницыPBR ImplementationBernie C. MagtalasОценок пока нет
- Mcqs Ethics and CSR)Документ9 страницMcqs Ethics and CSR)Maida TanweerОценок пока нет
- Philippine Phoenix Surety & Insurance, Inc. Vs Woodworks, Inc Digest - MungcalДокумент1 страницаPhilippine Phoenix Surety & Insurance, Inc. Vs Woodworks, Inc Digest - Mungcalc2_charishmungcalОценок пока нет
- Risk Management GuidanceДокумент9 страницRisk Management GuidanceHelen GouseОценок пока нет
- PIL HANDOUT in TextДокумент173 страницыPIL HANDOUT in Textbhargavi mishraОценок пока нет
- c15 ldn01610 SchematicДокумент4 страницыc15 ldn01610 SchematicJacques Van Niekerk50% (2)
- New CVLRДокумент2 страницыNew CVLRanahata2014Оценок пока нет
- Sales Force TrainingДокумент18 страницSales Force Trainingsaurabh shekhar100% (2)
- SYKES - Telework Work Area AgreementДокумент2 страницыSYKES - Telework Work Area AgreementFritz PrejeanОценок пока нет
- LCD Television Service Manual: Chassis MTK8222 Product TypeДокумент46 страницLCD Television Service Manual: Chassis MTK8222 Product TypetvdenОценок пока нет