OMB Approval No.
APPLICATfON FOR 2. DATE SUBMITTED
Applicanllder -er
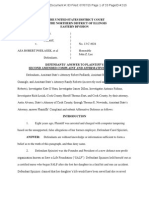
FEDERAL ASSISTANCE
April 13, 2004 J?A# 04164
1. TYPE OF SUBMISSION: 3. DATERECEIVEDBVSTATE
State Application Identifier
Appi;calion Preappliczllion
r Constn.clicn
4. DATe RECEIVeD BY FEDERAl. AGENCY
Fedelalldentifier
I>(
S. APPUCANT INFORMAnON
Legal Name: Organizationaluntt
Save A Life Foundation
.Aclclnm (glw ely. COUIII)', uto, IMifl ZiP r:/of.
Nam!J an<SIMpl1oM numb8l' oiii'IO porscn 10 bo con1a1:1oc1 on matlflrs Involving 1t11s Oflllliealiclft
O'Hare Aerospace Center
(givP /!IIJII C<Kio}
9950 West Lawrence Ave. Ste #300
carol J. Spizzirri President/Founder
Schiller Park, Illinois 60176
(847) 9289683
S. BIPLOYER IDf:HnFICAT&ON NUMBER (EJN):
7. TYPE OF APf>UCAHT: (en tor apptDpdara 111!11/r In box}
[;]
A. Slate H. IMepenclotrl School Oist.
&. B.Ccunty I. StaCa Con:tacodlnsi!Mian ol HigMt Laaming
r ConllnrmUon r Revision
C. Mtll\lcipal J . Pr\vala 1Jniv4rally
D. Township K.tndianTdb&
0 D
E. tntersllllo
'- lndMdual
U Revision. enutt apptgpllalo IDUarts) in box(os}:
F. lmomwnlc:ipal M. Ptolil Organimtion
G. Distll;l N. Othar {Spst:;ily):
A. lnc:roiiSo Awan! B. Oecmau Awanl c. Increase OuteliOn
0. Ooc:nia.se Duntlion Othur (sptiCi!yj: 9. NAME OF FEDERAL AGENCY:
Centers For Disease COntrol & Prevention
10. CATALOG OF FEDERAL DOMESTIC 11. DESCRIPTIVE TITLE OF APPUCANT'S PROJECT:
ASSISTANCE NUMBER:
rn-1 I I I
Expand The Training Of Basic Life
Support and Emergency Preparedness
nnE; Skills, especially to children
12. AREAS AFFECTED BY PROJECT (CiliD$. COUIIIias, Sla!H,IIIC.):
IL, WI, NC, NY, FL, PA,
13. PROPOSED PROJECT:
14. CONGRESSIOtlAL DISTRICTS OF:
Stan Date EncfmgData a. Appttcant .b. ProJect
06/01/04 05/31/05 Cook County, IL
-
Dist. Earmark for Save A Life
ll,lO,lS,l4, 19 Foundation
15. ESTIMATED FUtlDING:
11. ISAPPUCATION SUBJECT TO REVII:W BY STATE EXEcunVE ORDER 12372 PROCESS?
a.. Federal
$ .00
a. YES. m5 PREAPPIJCATIONIAPPUCATION WAS MADE AVAILABLE TO THE STATE EXECUTIVE
1,005,000 ORDER 1Z372 PROCESS FOR REVIEW ON:
b. Applicant $ .00
DATE
c. State
$ .00
d. Local
$ .00
b. NO.j5( PROGRAM IS NOT COVERED BY E.O. 12372
e. Other
$ .00
r OR PROGRAM HAS NOT BEEN SELECTED STATE FOR REVIEW
f. Program Income
$ .00
17. IS APPUCAnON DEUNOUENT ON ANY FEDeRAl.. DEST?
rves II "'M.: altllell an Ul)lallaUOn.
r
g. TOTAL
$ .00
1,005,000
18. TO THE BEST OF flY KNOWI.SCGE AND 8l!UEF, ALL DATA IN THIS APPIJCAnONIPREAPPUCATlON ARE TRUE AND CORRECT, THE OOCUMEHl' HAS BEEN DULY AIITHORIZCO
BY THE GOVERNIHG BODY OF THE APPUCAHT AND lHE APPUCANT WILL CO!IIPI. Y wmf TME ATTACHED ASSURANCES IF THE ASSISTANCE IS AWARDED.
a. Typed Natne of Authorized Representative b. nue c. Telephone number
J. Spizzirri President/Founder 847-928-9683
?lf j
e. Date Signed
04/13/04
Editions ,W
I
StandatO Form 424 (Rev. 797)
Authorized for Local eprodu ton Prescribed by OMS Cilt:ular A102
PHS-5161-1 {7/00)
PagelS
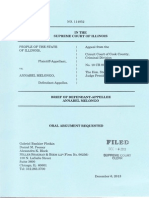
CHECKLIST OMB Approval No. 0920-0428
Public Burden Statement: Public reporting burden of this Clearance Officer, 1600 Clifton Road, MS D-24, AUanta, GA 30333,
collection of Information Is estimated to average 4 hours per ATIN: PRA (0920-0428). Do not send the completed form to this
including the time for reviewing in:;tructlons, searching address.
data sources. gathering and maintalmng the data needed,
and completing and reviewing the collection of infonnation. An NOTE TO APPUCANT: This form must be completed and
agency may not conduct or sponsor. and a person is not required to submitted with the original of your appfacation. Be sure to complete
respond to a collection of Information unless it displays a currently both sides of this form. Check the appropriate boxes and provide
valid OMB control number. Send comments this burden the Information requested. This form should be attached as the last
estimate or any other aspect of this collection of information, page of the signed original of the application. This page is reserved
including suggestions for reducing this burden to CDC, Project for PHS staff use only.
Type of Application:
Noncompeting Competing
r Continuation r Continuation r Supplemental
PART A:. The following checklist Is provided to assure that proper signatures, assurances, and certifications have bean submitted.
Included
NOT
Applicable
1. Proper Signature and Date for Item 18 on SF 424 (FACE PAGE) ........................... ..
2. Proper Signature and Date on PHS-5161-1 certifications page ...................... ...... .
3. Proper Signature and Date on appropriate "Assurances page, i.e.,
SF-4248 (Non-Construction Programs) or SF-424D (Construction Programs) .........
4. If your organization currently has on file with DHHS the following assurances,
please identify which have been filed by indicating the date of such filing on the line
provided. (All four have been consolidated into a single fonn, HHS Form 690)
IX
!X
IX Civil Rights Assurance {45 CFR 80) ...................... ............. ..... -----------
IX Assurance Concerning the Handicapped (45 CFR 64 ) .. .......... ------------
Assurance Concerning Sex Discrimination (45 CFR 86) ......... ------------
IX Assurance Concerning Age Discrimination (45 CFR 90 &
45 CFR 91) ...................................................... ..................... ..
5. Human Subjects Certification, when applicable {45 CFR 46) .................................... . r
PART B: ThJs part Is provided to assure that pertinent Information has been addressed and Included In the application.
r
NOT
YES Applicable
1. Has a Public Health System Impact Statement for the proposed program/project
been completed and distributed as required? ............................................................. ..
2. Has the appropriate box been checked for item# 16 on the SF-424 (FACE PAGE)
regarding intergovernmental review under E.O. 12372? (45 CFR Part 100) .............. .
3. Has the entire proposed project period been identified in item# 13 of the FACE
PAGE? ..................................................................................................................... .. .. .
4. Have biographical sketch(es) with job description(s) been attached, when
required? ......................................................... ........................................... ................... .
5. Has the "Budget Information page, SF-424A (Non-Construction Programs) or
SF-424C (Construction Programs), been completed and included? ........................... .
6. Has the 12 month detailed budget been provided? .............. .. ........ - ..................... ... .. ..
7. Has the budget for the entire proposed project period with sufficient detail been
provided? .................................................. ............... ............................... ................ ..... .
8. For a Supplemental application, does the detailed budget address only the additional
funds requested? .................. ... .... ..... ....................... .............................. ............ ..... ..... .
9. For Competing Continuation and Supplemental applications, has a progress report
been included? ..................... ....................................................................................... .
PART C: In the spaces provided below, please provide the requested Information.
r
j)(
P<
r
IX
)X
IX
r
r
r
r
IX
IX
Business otriCial to be noli1'1ed if an awam is to be made. Program Director/Project Direc:!ar/Principallnvestigator designated to
dlr&cllhe orcoosed DrOiect or DIOOtam.
Name Carol J . Spizzirri
nue President/Founder
OtgantzaUon Save A Life Foundation
9950 West Lawrence Ave. Ste#300
Schiller Park, IL 60176
Telephono Number ( 84 7) 928- 96 83
Fax Number ( 8 4 7 ) 512 9 - 9 6 64
Name Carol J. Spizzirri
nuo President/Founder
Organization Save A Life Foundation
9950 West Lawrence Ave Ste #300
Schiller Park, IL 60176
E-mail Address carolsalf. org
Telephone Number { 84 7} 92 8-96 83
Fax Number ( 84 7} 9.2 8-96 84
APPUCAHT ORGAHIZAnON'S 12-0IGIT DHHS EIN (If atrcacl)' SOCIAL SECURITY NUMBER HIGHEST DEGREe EARNED
c c I
J RN BS
(OVER]
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
PUBLIC HEALTH SERVICE
GRANT APPLICATION
For use by:
State and Local Government Applicants
Nongovernmental Applicants for Health Services Projects
----
Unable to load image
filter library
Status : 1157
FORM PHS-5161-1
(Revised 7 /00)
.. )
j
DEPARTMENT OF HEALTH & HUMAN SERVICES
Public Health Service
Centers For Disease Control
and Prevention (CDC)
Carol Spizzirri, President/Founder
Save-A-Life Foundation, Inc.
9950 West Lawrence Ave Suite 300
Schiller Park, IL 60176-1216
Reference: PA# 04164, Earmark for Save a Life Foundation
Dear Ms. Spizzirri:
y;:
The Save-A-Life Foundation has been identified to receive a CDC assistance award for
approximately $1,018,829. The budget period is expected to be from June 1, 2004 through
May 31,2005. Although you were funded a grant award under another program
announcement, you will receive a new one-year award under Program Announcement
Number 04164.
The purpose of the earmark funds is to evaluate the effectiveness ofthe Save-A-Life
training program and to implement and expand state training sites to a national training
capacity. This funding will be used for all costs associated with expansion of training sites
and evaluating the program.
In order to process the you must submit an application package. This letter is
designed to provide the guidance required to prepare the application package. Please read
and follow all the instructions below.
The application package must arrive this office no later than April 16, 2004. The
application packet should consist of an original plus 2 copies of the following:
Cover Letter that includes the names of the program director/principal
investigator's (PI) and business name, title, complete mailing address,
phone number, and email address. Also, provide a point of contact name ofperson
who prepared the application package, if different from PI.
PHS Form 5161. To obtain instructions and a tillable .copy of this form on line,
visit the following website: http://www.psc.gov/forms/FF99/PHS-5161-llphs-
5161-l.html. Clearly reference the PI ogram Announcement number on the
application. Number all pages including appendices. Print on only one side of each
page. Use single spacing. Do not staple or bind your application
)
SF 424. Within the website for the PHS Fonn 5161 are the SF 424's. Ensure the
amount entered on the SF-424 matches the Budget Narrative and detailed budget.
2
Important Note: Be sure to include the complete EIN for your organization,
including the two-digit suffu:. If you have never applied for assistance and do
not have an EIN, please be sure to note that in your cover letter. Also, you are
required to have a Dun and Bradstreet Data Universal Numbering System (DUNS)
number to apply for a grant or cooperative agreement from the Federal government.
Your DUNS number must be entered on the face page of the application form next
to the EIN. The DUNS number is a nine-digit identification number, which
uniquely identifies business entities. Obtaining a DUNS number is easy and there is
no charge. To obtain a DUNS nwnber, access www.dunandbradstreet.com or call 1-
866-705-5711.
Program Narrative. The following information is provided to assist you in
preparing your program narrative:
-Program Goals and Objectives. Provide a plan of action that describes the
proposed program objectives and activities for the upcoming budget period. Each
activity should lead to the accomplishment of the proposed objectives. Each
, objective must contain a performance or outcome measure that assesses the
effectiveness of the project. The applicant should adequately describe how it would
implement the program activities and disseminate the outcomes of the activities and
services provided. The application should include a detailed timeline for each
accomplishment.
-Program Requirements.
Detailed budget and justification. Up to $1 ,018,829 is available to fund this
award. Please prepare a budget that does not exceed this amount (including direct
and indirect costs). A sample budget template is located at the following website:
http://www .cdc. gov/od/pgo/fundinglbudgetguide.hnn.
Indirect Rate Agreement. Enclose a copy of your organization's most current
negotiated Federal indirect cost rate agreement. Note: Unless a cost rate agreement
has been federally approved by the Division of Cost Allocation, all budget items
should be direct costs.
Other Information:
Final Progress Report (within 90 days after the end "of the project period)
Final Financial Status Report (within 90 days after the end of the project period)
Applications may not be submitted electronically at this time. Please mail application
packet to the following address:
Angie Tuttle, Grants Management Specialist
Acquisition and Assistance Branch A
Centers for Disease Control and Prevention
2920 Brandywine Road, Mailstop K-75
Atlanta, GA 30341-4146
If you need any programmatic guidance, please contact J acqui Butler by telephone at
(770) 488-1496 or by email at JAButler@cdc.gov. If you need any budget guidance,
please contact me by telephone at (770) 488-2719 or by email at aen4@cdc.gov.
cc: Robin Forbes
Sincerely,
J T ~
Tuttle
G anagement Specialist
Acquisition and Assistance, Branch A
Procurement and Grants Office
3
. . \
SALF'
Carol J. Spizzirri
Founder I President
Save A Life Foundation
Tuesday,Apnl13,2004
Angie Tuttle Grants Management Specialist
CDC Centers For Disease Control & Prevention
Acquisition and Assistance Branch A
2920 Brandywine Rd, Mailstop K
Atlanta, GA 30341-4146
DUN# 08-092-0437
Re: Program Announcement PA #04164 Earmark for Save A Life Foundation
National Headquarters
99SO W. Lawrence Ave Ste 300
Schiller Park, Illinois 60176-1216
Ph: (847) 928-9683
F:u: (847) 928-9684
Toll Free: (888) 892-0606
Website: www.salf.org
Grant title: Expand The Training Of Basic Life Supporting and Emergency Preparedness Skills
Dear Ms. Tuttle:
Save A Life Foundation is a 501 C (3} organization dedicated to working with the public health
infrastructure to ensure the creation of a safety net for everyday citizens in the their communities. We
train citizens in life supporting first aid skills, with a particular focus on children (K-12} in age appropriate
programs that include i.e., Heimlich Maneuver, CPR, bleed control, blood borne- bio hazardous
precautions, access EMS, deployment of AED's_ Since 1997 SALF has trained nearly 1 million children in
Illinois, moving into Wisconsin in 2003 and are about to expand our system of training into even more
emergency and public health departments which SALF establishes its branch sites_ Using their local
emergency medical service providers as our instructors we are able to train children K-6th grades our
Save A Life For Kids program (1 hour), and 7th to 12th graders our Bystander Basic program (2 hours)
with remarkable success, both in skills retention and increased willingness by these same students to aid
the injured or ill at a time of an emergency. The proof of this accomplishment is due to our web base
data collection system participated by each student.
GRANT ACTIVITIES
In order for SALF to expand its base site in each targeted state SALF must:
- Locate a hospital to home a branch
Find and train an individual with EMS credentials to serve as a Facilitator
Obtain support from a physician to serve as Project Medical Director
Obtain support of local mayors to establish a Citizen Corps Council and apply for funds to
support the school training
Identify EMS providers and train as instructors
Identify local corporations willing to Adopt A School to defer training costs
Identify schools, schedule classes between schools and Instructors
Evaluate class and test students for skills proficiency
Each Instructor receives compensation for their travel and time which aids greatly in supplementing their
meager professional income while off duty.
Page2
Save A Life Foundation
April 13, 2004
Over the years SALF has been embraced by many including being the second affiliate of the U.S.
Homeland Security's Citizen Corps in January 2003, Illinois Homeland Security's Terrorism Task Force,
2001 and alike. Our partners include the U.S. Conference of Mayors, State Municipal Leagues, Chicago
Bar Association, Chicago Public Schools, Global Ronald McDonald's House Charities, and so forth.
My greatest pleasure besides seeing the children's faces as they discover their new ability to save a life,
working with CDC since 2001, is serving with Dr. Peter Safar (Father of CPR) and Dr. Henry Heimlich
(Heimlich Maneuver) SALF's founding Medical Board, to train the critical mass should they faced an
emergency.
Everyone has a emergency role. The "Pre-EMS" role is the most crucial in maintaining life until advance
EMS arrives. SALF feel fortunate that CDC feels the same.
encl.
Вам также может понравиться
- Donald John Angelini, JR., Files Appearance On Behalf of Carol SpizzirriДокумент1 страницаDonald John Angelini, JR., Files Appearance On Behalf of Carol Spizzirrianacondakay044Оценок пока нет
- Cook County Defendants' Answer and Affirmative Defense in Melongo's Civil Right CaseДокумент34 страницыCook County Defendants' Answer and Affirmative Defense in Melongo's Civil Right Caseanacondakay044Оценок пока нет
- Jennifer Bonjean Motion To Request Default Judgment Against Carol Spizzirri and Mathew MarkosДокумент8 страницJennifer Bonjean Motion To Request Default Judgment Against Carol Spizzirri and Mathew Markosanacondakay044Оценок пока нет
- 2/23/15 Schiller Park Further Support For Motion To DismissДокумент5 страниц2/23/15 Schiller Park Further Support For Motion To DismissPeter M. HeimlichОценок пока нет
- Motion To Set Aside Default Judgment Against Carol Spizzirri in Melongo's Civil Right CaseДокумент6 страницMotion To Set Aside Default Judgment Against Carol Spizzirri in Melongo's Civil Right Caseanacondakay044Оценок пока нет
- Annabel K Melongo Response To Cook County Motion To DismissДокумент12 страницAnnabel K Melongo Response To Cook County Motion To Dismissanacondakay044Оценок пока нет
- Annabel K Melongo Response To Illinois Attorney General Motion To DismissДокумент7 страницAnnabel K Melongo Response To Illinois Attorney General Motion To Dismissanacondakay044Оценок пока нет
- Melongo's Amended ComplaintДокумент21 страницаMelongo's Amended Complaintanacondakay044Оценок пока нет
- Second Amended ComplaintДокумент26 страницSecond Amended Complaintanacondakay044Оценок пока нет
- Schiller Park Motion To Dismiss Annabel Melongo Civil Right Case 13cv04924Документ16 страницSchiller Park Motion To Dismiss Annabel Melongo Civil Right Case 13cv04924anacondakay044100% (1)
- Melongo's Eavesdropping Appeal Brief at The Illinois Supreme CourtДокумент60 страницMelongo's Eavesdropping Appeal Brief at The Illinois Supreme Courtanacondakay044Оценок пока нет
- Motion To Recuse Appoint ProsecutorДокумент21 страницаMotion To Recuse Appoint Prosecutoranacondakay044Оценок пока нет
- Eavesdropping Notice of AppealДокумент2 страницыEavesdropping Notice of Appealanacondakay044Оценок пока нет
- Melongo's Motion Requesting Judge Goebel To Reconsider His 10-25-12 Ruling Denying Her MotionДокумент8 страницMelongo's Motion Requesting Judge Goebel To Reconsider His 10-25-12 Ruling Denying Her Motionanacondakay044Оценок пока нет
- Melongo's Appendix From Her Eavesdropping's Brief at The Illinois Supreme CourtДокумент53 страницыMelongo's Appendix From Her Eavesdropping's Brief at The Illinois Supreme Courtanacondakay044Оценок пока нет
- Cook County Plaintiff-Appellant's Brief in People v. Melongo CaseДокумент30 страницCook County Plaintiff-Appellant's Brief in People v. Melongo Caseanacondakay044Оценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Combustible Dust AwarenessДокумент33 страницыCombustible Dust AwarenessDSG100% (1)
- JR Automation Technologies Emergency Action Plan Published June 2014Документ15 страницJR Automation Technologies Emergency Action Plan Published June 2014api-254303808Оценок пока нет
- 2nd Lesson PlanДокумент7 страниц2nd Lesson PlanMarlon James TobiasОценок пока нет
- 52 (Consequence Analysis)Документ18 страниц52 (Consequence Analysis)Aditya PranotoОценок пока нет
- Computer Aided Structural AnalysisДокумент149 страницComputer Aided Structural AnalysisDeepak PandeyОценок пока нет
- March 2010 ACECOMS Magazine 15th AnvДокумент52 страницыMarch 2010 ACECOMS Magazine 15th AnvKazi MamunОценок пока нет
- Earth-Science PETA 4TH QUARTERДокумент1 страницаEarth-Science PETA 4TH QUARTERReydric DavidОценок пока нет
- Climate Change Impacts, Vulnerability and Adaptation in ZimbabweДокумент40 страницClimate Change Impacts, Vulnerability and Adaptation in ZimbabweBrighton MugutaОценок пока нет
- Internship ReportДокумент50 страницInternship ReportBishnu Dhamala71% (14)
- ISO 22301 ChecklistДокумент2 страницыISO 22301 ChecklistAhmed M. SOUISSIОценок пока нет
- Padre Garcia Conplan 2019 EARTHQUAKEДокумент18 страницPadre Garcia Conplan 2019 EARTHQUAKERey Mark Collado100% (2)
- JNPTPDFEmergency Action Plan458 PDFДокумент133 страницыJNPTPDFEmergency Action Plan458 PDFAnonymous fpLGbRDlОценок пока нет
- IT Audit of Manthan System in Indian Oil Corporation LimitedДокумент32 страницыIT Audit of Manthan System in Indian Oil Corporation LimitedManish JangidОценок пока нет
- Is 800 2007Документ300 страницIs 800 2007Deepak MeenaОценок пока нет
- BP Oil Spill BBC News TimelineДокумент6 страницBP Oil Spill BBC News TimelineKing ShakzОценок пока нет
- Perida, ShelouДокумент60 страницPerida, ShelouNickCanabeОценок пока нет
- Pet 411 Group Report UgoДокумент9 страницPet 411 Group Report UgoUgo UmeojiakuОценок пока нет
- Sop BorewellДокумент28 страницSop BorewellAjay kumarОценок пока нет
- 9/11 AttackДокумент17 страниц9/11 AttackJames BradleyОценок пока нет
- A.2 2017 - ISO Folder Front Label - RUДокумент6 страницA.2 2017 - ISO Folder Front Label - RUJan Lawrence AlbertoОценок пока нет
- NSTPДокумент3 страницыNSTPFrances Patricia TimbangОценок пока нет
- CG Information BrochureДокумент60 страницCG Information BrochureSaumya MohanОценок пока нет
- Decommissioning A System White PaperДокумент6 страницDecommissioning A System White PaperYajurvedi TabibОценок пока нет
- Sample AttachmentДокумент8 страницSample AttachmentMildred VillarubiaОценок пока нет
- Group3 Action PlanДокумент6 страницGroup3 Action PlanMichaelОценок пока нет
- Concap Logcap Afcap Smart BookДокумент29 страницConcap Logcap Afcap Smart BookJohn NguyenОценок пока нет
- Jose, Kathlyn Mae - Final Requirement - NSTP 2 - ACT225Документ23 страницыJose, Kathlyn Mae - Final Requirement - NSTP 2 - ACT225Darren Dela Cruz CadienteОценок пока нет
- AISC Seismic Design Module1 Introduction V2Документ103 страницыAISC Seismic Design Module1 Introduction V2Shantonu DeyОценок пока нет
- FEMA 451 - NEHRP Design Examples 2006Документ860 страницFEMA 451 - NEHRP Design Examples 2006Halleith1875100% (5)
- Room Discount FormДокумент1 страницаRoom Discount FormMeriem DjeОценок пока нет