International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
47
TQM HEALTH PRACTICES AND CLIENT SATISFACTION IN A
SELECTED HEALTH FACILITY IN GHANA
George O. Mainoo
1
, Bright Addo
2
, Adu Gyamfi Boadi
3
1, 2
Department of Sociology and Social Work,
3
Institute of Distant Learning,
Kwame Nkrumah University of Science and Technology, Ghana
ABSTRACT
Total Quality Management (TQM) for health care delivery provides a model to help hospitals
organize, communicate, monitor, and continuously improve all aspects of health care delivery. The
literature concerning service quality dimensions in the healthcare industry is replete with studies
from the developed world. Researchers from developing countries are yet to fully demonstrate the
impact of TQM health practices on client satisfaction. The current study aimed to establish the TQM
health practices (adequacy of health facility and health care amenities, doctor-patient relationship,
pharmacy staff service delivery, and nurses and midwives service delivery) that determine client
satisfaction in a selected Health facility in the Ashanti Region of Ghana. The design of the study was
a cross-sectional survey of 150 patients between the ages of 18 - 60+years who were sampled
randomly. The sample consisted of 72 male (48%) and 78 female (52%) clients. We used Pearson
product moment correlation coefficient and Multiple regression models for analysis. Results of the
correlation analysis revealed that, condition of health facility, doctor-patient relationship, and nurses
and midwives service delivery significantly relates to client satisfaction of health care delivery (r =
0.261, 0.348 and 0.638; p = 0.001, 0.000 and 0.000 respectively). The Standard multiple regression
analysis also revealed that only nurse and midwives service delivery is a unique and statistically
significant predictor of clients satisfaction. We recommend consistent review of health care
practices that seek to promote the positive correlate in this study to enhance sustenance and growth
in health care delivery in Ghana.
Keywords: Total Quality Management, Health Practices, Clients, Health Facility, Satisfaction,
Ghana.
BACKGROUND
Good health, responsiveness to the expectations of its people, and financial contribution to
the nation are the goals for health care systems of any country (WHO, 2000). An overview of the
INTERNATIONAL JOURNAL OF MANAGEMENT (IJM)
ISSN 0976-6502 (Print)
ISSN 0976-6510 (Online)
Volume 5, Issue 8, August (2014), pp. 47-56
IAEME: http://www.iaeme.com/IJM.asp
Journal Impact Factor (2014): 7.2230 (Calculated by GISI)
www.jifactor.com
IJM
I A E M E
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
48
health scenario all over the world indicates that despite having numerous excellent health care
facilities, there exists a sufficiently large gap between the demand and quality of health care delivery.
The past two decades in the health care delivery system in Ghana have seen health care
professionals, technicians and clients/patients alike having a lot of issues to grumble over. Patients or
clients health care has in times of health professionals agitations and industrial strike being kept in
limbo. The level of trust and confidence in the health care delivery system has indeed become an
issue to ponder over. However, not many studies have been conducted in this area of rear health
crisis in the government or private hospitals in Ghana.
A comparative analysis of the mortality and morbidity patterns of pre-colonial, colonial and
post-colonial periods presents a gloomy picture of the health status and systems of the nation (Senah,
2001). Generally, while Ghanaians now live longer (60-years) the causes of mortality and morbidity
have not been significantly controlled given the huge capital outlay the country has made and
continues to make on improving healthcare service delivery (GDHS, 2008; Senah, 2001). The
analysis of health status indicators in Ghana points to a nation in crisis.
The statistics indicate that although about 69 percent of the population lives in rural
communities, only 3 percent of rural households live in communities where there is a doctor; for 36
percent of rural households, a doctor is about 15 km away and for 18 percent a doctor is about 50km
away. Forty-four (44) percent of doctors are located in the Greater Accra Region, which
accommodates only 18 percent of the national population. The doctor-patient ratio is 1:11,929 while
that of nurses is 1:971 (GHS, 2010). Maternal mortality rate is currently put at 350 deaths/100,000
live births (CIA World Fact book, 2012). Infant/child mortality rate is also put at 41 deaths/1000 live
births (CIA World Fact book, 2013). For developing economies, like that of Ghana, the provision of
health care is always problematic. Although there is a greater recognition that health care is a basic
need of life that must be improved and sustained to all Ghanaians, the practical problems
encountered in the implementation of this objective require moral aptitude and commitment in the
political economy (see Senah, 2001). Where resources are limited, it is difficult deciding how best to
use them for development; and that implies difficulty in sustainability also.
In Africa where economic dependency is the norm, policy makers are constantly faced with the task
of making choices which are economically, socially and morally defensible although, but perhaps are
politically expedient as well. This situation calls for a rational clarion call to adopt the principle of
Total Quality Management practices to increase efficiency and maximize utilisation of the scare
resource of the nation.
Juran (1995) defines TQM as the system of activities directed at achieving delighted
customers, empowered employees, higher revenues, and reduced costs. It is a philosophy aimed at
continuously improving the quality and process to achieve customer satisfaction of service
(Stevenson, 2002). Simply put, it is the building of quality into products and process of making
quality a concern and responsibility for everyone in an organization or institution (McAdam, 2000).
Studies have suggested quite a large number of factors/elements/constructs/dimensions of TQM
implementation. TQM and performance improvement have a positive relationship, particularly, the
Malcolm Badrige quality award criteria confirms such relationship between quality management
practices and business results (Heidari, Gorji & Farooquie, 2011). A study by Salaheldin (2009)
indicates that there are many empirical studies which examine TQM practices performance
relationships in large firms but the health sector has received less attention by researchers. While the
literature concerning service quality dimensions in the healthcare industry is replete with studies
from the developed world, researchers from developing countries have been exploring the
applicability of the related models and frameworks in their specific context (Heidari, Gorji &
Farooquie, 2011). The wholesale adoption of developed world models is inadequate to transform and
improve TQM practices in Ghana.
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
49
Ghana does not seem to have any established framework for measuring quality efforts and
performance of its health care industry. Zakuan et al. (2010) suggest that despite the number of
publications and quantity of research on TQM, there is actually little empirical work that has been
carried out in developing countries, particularly in the ASEAN region and Sub-Sahara Africa. There
are evidences of recent studies in developing countries such as India and Iran pertaining to total
quality management and performance in health care (Duggirala, Rajendran & Anantharaman, 2008;
Padma, Rajendran & Sai, 2009: Maleki & Izadi, 2008), however, none of them claims for having
addressed the issue in totality. The current state of research in the area of health care quality along
with the inadequacy and cost of health care services in Ghana justifies the conduct of this study.
Several non-Ghanaian studies have identified one or more practices that contribute to
improvement in the quality of healthcare delivery (e.g. Maleki & Izadi, 2008; Duggirala, Rajendran
& Anantharaman, 2008; Padma, Rajendran & Sai, 2009), however, there is no study to date that has
examined the TQM for healthcare delivery in relation to TQM health practices such as: condition of
health facility, doctor-patient relationship, pharmacy staff service delivery and nurses and midwives
care as predictor variables in the Ghanaian context.
AIMS OF STUDY
The aim of this study was to identify a set of TQM health practices that predict clients
satisfaction and that which are helpful in improving the overall quality of healthcare.
The study also aimed to determine the relationship between: condition of health facility, doctor-
patient relationship, pharmacy staff service delivery and nurses and midwives care as TQM health
factors and client satisfaction as an outcome variable.
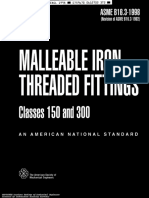
Conceptual Model
Source: Authors own creation (2013)
Figure 1.0: Conceptual model of TQM health practices that influence their implementation in
healthcare delivery System in Ghana
Improved
Quality of
Healthcare
Delivery
State, level and
Adequacy of
Hospital
Amenities
TQM
Implementation
Doctor-Patient
Relation
Research,
Development,
Education, Culture
and NHIS
Government
and Stakeholder
Appraisal and
culture
Client
Satisfaction
Attitude, Adequacy
and Competency of
Health care delivery
Professionals
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
50
Design and Methods
The design of the study was a cross-sectional survey which utilized a probability sample with
a structured questionnaire for the collection of quantitative data involving multiple variables that
were examined to detect patterns of relationship and associations. In using this design, we were able
to collect data on more than one case at a single point in time.
Study Population and Sample
The population of the study consisted of patients who reported for medical care at a public
health care facility in the Ashanti Region. One hundred and fifty (150) patients were, however
randomly sampled for the study. The sample size (n=150) was informed by the formula given by
Tabachnick and Fidell (2007) in calculating the adequate sample for multiple regression analysis.
Taking into account the number of independent variables one wishes to use, the formula is given as:
N > 50 + 8m (where m = number of independent variables). Since this study made use of four
independent variables the number of cases required was 82. The 150 patients sampled for the study
was therefore adequate to perform the multiple regression analysis.
Variables and Measures
The dependent variable in this study was client satisfaction. The independent variables were:
condition of health facility, doctor-to-patient relationship, pharmacy staff service delivery and nurses
and midwives care.
Client Satisfaction
Client satisfaction was assessed by one item with a five point scale (1= Poor to 5= Excellent)
regarding the overall assessment of medical care provided by the hospital. Patients assessed this item
by circling the number that corresponded to the degree to which they agreed to the statement
provided. On this scale higher scores indicated quality healthcare delivery.
Condition of Health Facility
Condition of health facility was assessed by nine (9) items using a rating scale of (1=
Strongly disagree to 5=Strongly agree) regarding the overall assessment of condition of facilities in
the hospital. Variables measured included; adequate ventilation at the reception rooms, clean hospital
premise, clean wards, clean toilets, reliability of ambulatory service, silence in ward and presence of
mosquitoes. Clients assessed these items by circling the number that corresponded to the degree to
which they agreed to the nine (9) statements on health conditions posed to them. The sum of the nine
(9) subscale items was taken as the measure of condition of health facility. The Cronbach alpha for
this subscale was 0.78.
Doctor-patient relationship
Six questionnaire items measured doctor-patient relationship. This variable was assessed on a
five point scale of 1=strongly disagree to 5=strongly. Items measured included: hours of waiting to
see a doctor, adequacy of time spent to discuss medical issues, maintenance of respect during
consultation and doctors explanation of clients condition. Like condition of health facility, patients
assessed these items by circling the number that corresponded to the degree to which they agreed to
the statement provided. The sum of all subscale items was taken as the measure of doctor-patient
relationship. On this scale higher scores indicated positive or good relationship between doctors and
patients. Cronbach alpha for this subscale was 0.81.
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
51
Pharmacy Staff Service Delivery
Pharmacy service delivery as a determinant of health service quality was assessed by three
items which included: friendliness of pharmacy staff, respectfulness of pharmacy staff and waiting
for long hours to collect medication. The three items measured pharmacy staff service delivery on a
5-point scale (1=Strongly disagree to 5=Strongly agree) The sum of all subscale items was computed
and the composite score used for analysis as pharmacy staff service delivery. A Cronbach alpha of
0.79 indicated that this subscale was also reliable.
Nurses and Midwives Care
Five items with a five point scale of 1=Strongly disagree to 5= Strongly agree was developed
to measure nurses and midwives service delivery. Items measured included; provision of assistance
to patients and pregnant women, respectfulness of nurses and midwives and proper care of pregnant
women in the ward. The scales of these five measures were transformed into a single measurement
sub-scale item, and the total sum used as a measure of nurses and midwives care. The Cronbach
alpha for this subscale was 0.82.
DATA COLLECTION AND ANALYSIS
Data was collected over a two day period after pre-test and post-test of the research
instrument had been carried out and the administrator of the facility had given his approval. Data
was obtained through the use of a structured questionnaire appropriately and specifically designed
for the study. Questionnaire items were placed under two main sections: background characteristics
of respondents and TQM health practices. Before the commencement of the study, permission was
sought from the Medical Director and Health Administrator of the hospital. Individual informed
consent was obtained from all participants before administrating the survey instrument. In order to
ensure anonymity of the study participants, they were instructed not to provide any form of personal
identification. The data collected was entered, cleaned and analysed using the SPSS (v20)
programme. Demographic characteristics of clients was analysed descriptively using frequency and
percentages. Based on the appropriateness, the study used Pearson correlation to determine the
possible relationship or association between measured TQM health practices and client satisfaction.
TQM health practices that significantly had an effect on client satisfaction were identified by
Standard Multiple Regression.
RESULTS
Demographic characteristics of the sample
The sample of the study was evenly distributed with respect to gender (48% male, 52%
female). Age distribution of the sample revealed majority of the clients being between the ages of 18
and 37 years (n=89, 59%). A total of 89 of our respondents sampled had obtained Tertiary level of
education with 10 of them not having attained any form of formal education. Data on the ethnic
background of respondents revealed the Akan tribe being the predominant ethnic group in the
sample. The marital status of respondents revealed majority of our respondents being married
(n=60). Respondents who were divorced were the least represented (n=9). Table 1.0 gives a
summary of the results on the demographic characteristics of the sample.
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
52
Table 1.0: Demographic characteristics of Patients
Variable N %
Sex
Male 72 48.0
Female 78 52.0
Age (years)
18 27 49 32.7
28 37 40 26.7
38 47 35 23.3
48 57 18 12.0
58+ 8 5.3
Level of Education
None 10 6.7
J.H.S 20 13.3
S.H.S 31 20.7
Polytechnic 43 28.7
University 46 37.0
Ethnicity
Akan 73 48.7
Ewe 22 14.7
Ga 27 18.0
Dagomba 23 15.3
Mamprusi 5 3.3
Marital Status
Single 46 30.7
Married 60 40.0
Separated 24 16.0
Divorced 9 6.0
Widowed 11 7.3
Source: Field Survey, March, 2013
Bivariate correlations for TQM health factors and client satisfaction
Significant positive correlations were found between all measures of TQM health factors and
client satisfaction (r = .26, p = 0.001 for condition of health facility; r = .35, p = 0.000 for doctor-
patient relationship; r = .28, p = 0.03 for pharmacy staff service delivery and r = .64, p = 0.000 for
nurses and midwives care).
Standard Multiple Regression Analyses for TQM health factors and Client Satisfaction
A standard multiple regression was performed between client satisfaction as dependent
variable and condition of health facility, doctor-to-patient relationship, pharmacy staff service
delivery and nurses and midwives service delivery as independent variables. We conducted the
regression analysis to determine the best linear combination of condition of health facility, doctor-to-
patient relationship, pharmacy staff service delivery and nurses and midwives service delivery for
predicting client satisfaction.
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
53
Results of the Standard multiple regression analysis revealed that the combination of
variables significantly predicted client satisfaction, F(4, 149) = 25.27, p < 0.001, with all four
independent variables contributing to the prediction. The model as a whole explained about 41%
(R
2
= 0.411) of the variation in client satisfaction. The beta weights, presented in Table 2.0 suggest
that nurses and midwives care is a significant predictor of client satisfaction.
Table 2.0: Simultaneous Multiple Regression analysis summary for TQM health factors
(independent variables) predicting Client Satisfaction (N=150)
Variable B SEB Sig.
(Constant) -.691 .449 .126
Condition of health facility -.005 .014 -.027 .716
Doctor-to-patient
relationship
.019 .025 .055 .458
Pharmacy staff service
delivery
-.005 .038 -.009 .898
Nurses and midwives care .251 .032 .628 .000*
Note. R
2
= .411; F(3, 149) = 25.27, *p < 0.05
From Table 2.0, nurses and midwives service delivery recorded the largest beta () value
(0.628) and also made a unique and statistically significant (p < 0.001) contribution to the prediction
of client satisfaction followed by doctor-patient relationship (0.055), with the lowest value of beta
recorded for pharmacy staff service delivery (-0.009). This means that nurses and midwives care
makes the strongest unique contribution to explaining the dependent variable (client satisfaction)
when the variance explained by all other variables in the model is controlled for. The lowest Beta ()
value recorded for pharmacy staff service delivery indicates that it made less of a unique
contribution.
DISCUSSION
Over all, the consistent patterns in the analyses of the results of the study tend to reflect the
findings of total quality management (TQM) of healthcare service delivery from the extant literature.
The results of the regression analysis revealed that of the four TQM health practices selected for the
study, only nurses and midwives care proved to be a significant determinant or predictor of client
satisfaction. Patients usually spend a lot of hospital time with nurses than they do with any other
worker in a hospital. It is therefore not surprising that the untoward behaviour of some nurses to
patients have come under so much criticism in recent times. The finding of nurses and midwives
service delivery having a significant effect on client satisfaction and quality health delivery as a
whole is supported by the studies of Boshoff and Gary (2004), Tucker and Adams (2001) and
Duggirala et al., (2008b).
Existing literature (e.g. McFadden et al., 2006; Yang, 2003) have reported that hospital
infrastructure significantly has an effect on healthcare delivery. Our study also sought to determine if
condition of health facility significantly related to client satisfaction of health care delivery. The
correlation results showed a positive and statistically significant association between condition of
health facility and client satisfaction. The implication of this result is that when condition of health
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
54
facility is improved, quality of healthcare will invariably be improved which would make clients
satisfied with the care they receive.
The positive and significant relationship between doctor-patient relationship and client
satisfaction established by the correlation analysis corroborates the findings of authors such as
Andaleeb (1998) and Gilbert et al., (1992) who also established that doctors care significantly
associate with healthcare delivery. The association between doctor-patient relationship and client
satisfaction of health care delivery implies that doctor-patient relationship significantly has
satisfactory effect on client satisfaction.
Consistent with the studies of Tucker and Adams, 2001, Gilbert et al. (1992) which found
services provided by nurses and midwives has a satisfactory effect on the healthcare delivery and
wellbeing of clients, our study also found a positive and significant relationship between nurses and
midwives service delivery and client satisfaction. The relationship between the two variables implies
that the service provided by nurses and midwives has an effect on healthcare delivery which
determines clients satisfaction.
CONCLUSION
Patients or client satisfaction is considered as a significant indicator of the quality of health
care provided by public or private hospitals the world over. The growing prominence of total quality
management (TQM) in health care was the basis of the present study to identify the set of TQM
health practices that significantly have an effect on client satisfaction. More specifically, this study
examined the relationship between conditions of health facility, doctor-patient relationship,
pharmacy staff service delivery, and nurses and midwives care and client satisfaction. The study
found a positive and statistically significant relationship between the selected TQM health factors
and clients satisfaction of quality of health care delivered. Consistent with existing findings, TQM
health practices put together has an influence on client satisfaction as indicated by the Multiple
regression analysis which also revealed that only nurses and midwives service delivery is the best
and most important predictor of client satisfaction of health care delivery.
Recommendation for Administrative Practice
For the successful implementation of TQM philosophy in the health care institution some of
the managerial implications of our study are:
Managers can use TQM philosophy as a strategic tool for achieving desirable outcome such
as patient satisfaction and improved quality of care.
Managers as well as quality policy makers in health care institutions should pay particular
attention to the vital role nurses and midwives play in the overall operations of the health
sector.
Finally, hospital administrators can understand the importance of satisfying all internal and external
stakeholders upon the introduction of TQM strategy.
Recommendation for Future Research
The scope and suggested direction for further research work in this area are:
A comparative study with other less developed countries may be carried out to observe the
similarities and dissimilarities concerning TQM implementation in health care institutions.
Further studies need to be undertaken concerning the detailed impact of identified health
practices of this study on TQM implementation.
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
55
Empirical research should be conducted to evaluate the understanding of the TQM practices
based on clients point of view.
LIMITATION OF THE STUDY
A major limitation of this study is its inability to generalize findings to the other healthcare
institutions in Ghana. Data collected for the study was peculiar to the selected health facility which
does not share the same health facilities with other hospitals in the country. The implication is that
different responses would have being obtained if the study was conducted in hospitals in other
regions of the country.
REFERENCES
[1] Andaleeb, S. S. (1998). Determinants of customer satisfaction with hospital: an managerial
model. International Journal of health care quality assurance, 11(6), 181-187.
[2] Boshoff, L. & Gray B. (2004). The relationships between service quality, customer
satisfaction and buying intentions in the privet hospitals industry. South African journal of
business management, 35(4), 27-37.
[3] CIA World Fact book, 2012 (Assessed on February 21, 2013).
[4] CIA World Fact book, 2013 (Assessed on February 21, 2013).
[5] Duggirala, M., Rajendran, C. & Anantharaman, R. N. (2008a). Patient-perceived dimensions
of total quality service in health care. Benchmarking International Journal, 15(5), 560-583.
[6] Duggirala M., Rajendran C. & Anantharaman R. N. (2008b). Provider-perceived dimensions
of total quality management in health care. Benchmarking International Journal, 15(6),
693-722.
[7] Faisal, T., Zillur, R., & Mohammed, A. (2011). Best practices of total quality management
implementation in health care settings, Health Marketing Quarterly, 28(3), 232-252,
DOI: 10.1080/07359683.2011.595643
[8] Ghana Health Service (GHS) Facts and Figures (2010).
[9] Gilbert F. W., Lumpkin J. R., Dant, R. P. (1992). Adaptation and customer expectations of
health care options. Journal of health care management, 12 (3), 46-55.
[10] Gorji, A. M. H., & Farooquie, J. A. (2011). A comparative study of total quality management
of health care system in India and Iran. BMC Research Notes, 4, 566
http://www.biomedcentral.com/1756-0500/4/566
[11] Juan, J. T. (2005). Components of successful total quality management. Emerald, 17
http://www.emeraldinsight.com/case_studies
[12] Maleki, M. R. & Izadi, A., (2008). Comparative study of results of two hospitals in Tehran
based on the organisational excellence model. Journal of Qazvin: Uni Med Sci Iran, 12(2),
63-68.
[13] McAdam, R: (2000). Three leafed clover?: TQM, Organisational excellence and business
improvement. TQM Magazine, 12(5), 314-320.
[14] McFadden, K. L., Stock G. N. & Gowen III C. R. 2006. Implementation of patient safety
initiatives in U.S. hospitals. International Journal of Operation and Production Management,
26 (3), 326-347.
[15] Padma, P., Rajendran, C., Sai, L. P. (2009). A Conceptual framework of service quality in
health care: perspectives of Indian patients and their attendants. Benchmark International
Journal, 16 (2), 157-191.
International Journal of Management (IJM), ISSN 0976 6502(Print), ISSN 0976 - 6510(Online),
Volume 5, Issue 8, August (2014), pp. 47-56 IAEME
56
[16] Salaheldin, S. I (2009): Critical Success Factors for TQM Implementation and their Impact
on Performance of SMEs. International Journal of Productivity and Performance
Management, 58(3), 215-237.
[17] Senah, K. A., (1989). Problems of the health care delivery system. In K.A. Ninsin and E.
Hansen, eds., The State, Development and Politics in Ghana. Dakar: Codesria Book Series.
Pp. 242 67
[18] Senah, K. A., (2001). In sickness and in health: globalization and health care delivery in
Ghana. Research Review NS 17.1, 83-89
[19] Stevenson, W. J (2002). Operations management. McGraw-Hill International Editions;
Seventh
[20] Tabachnick, B. G. & Fidell, L. S. (2007). Using multivariate statistics (5th edn). Boston:
Pearson Education.
[21] Tucker, J. & Adams S. R. (2001). Incorporating patients assessments of satisfaction and
quality: an integrative model of patients evaluation of their care. Managing service quality,
11(4), 272-286.
[22] World Health Organisation (WHO). (2000). The World Health Report 2000Health systems:
improving performance.[http://www.who.int], accessed on May 10, 2013.
[23] World Health Organisation (WHO). (2010). Evaluation of Recent Changes in the Financing
of Health Services: A Report of a WHO study Group. WHO Technical Report Series Geneva.
[24] Yang, C. C. (2003). The establishment of a TQM system for the health care industry. The
TQM Magazine, 15(2), 9398.
[25] Zakuan, N. M., Yusofb, S. M, Laosirihongthong, T., Shaharounb, A. M (2010). Proposed
relationship of TQM and organisational performance using structured equation modelling.
Total Quality Management, 21(2), 185-203.
[26] R. Thiru Murugan and Dr. J Clement Sudhahar, Predictors of Customer Retention in Online
Health Care System (OHCS) - Structural Equation Modelling (SEM) Approach,
International Journal of Management (IJM), Volume 4, Issue 1, 2013, pp. 243 - 257,
ISSN Print: 0976-6502, ISSN Online: 0976-6510.
[27] Dr. Satpal Singh and Dr. Sahil, Study on Medical Tourism Global Competition in
Healthcare and a Study on Satisfaction Level Among Foreign Patients, International
Journal of Marketing & Human Resource Management (IJMHRM), Volume 5, Issue 1, 2014,
pp. 9 - 21, ISSN Print: 0976 6421, ISSN Online: 0976- 643X.
[28] B.Sambath Kumar and Dr.S.S.Rau, A Study on Service Oriented Architecture in Electronic
Patient Health Record System, International Journal of Management (IJM), Volume 3,
Issue 1, 2012, pp. 165 - 168, ISSN Print: 0976-6502, ISSN Online: 0976-6510.
Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Broad Unexposed Skills of Transgender EntrepreneursДокумент8 страницBroad Unexposed Skills of Transgender EntrepreneursIAEME PublicationОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Determinants Affecting The User's Intention To Use Mobile Banking ApplicationsДокумент8 страницDeterminants Affecting The User's Intention To Use Mobile Banking ApplicationsIAEME PublicationОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- A Study On The Reasons For Transgender To Become EntrepreneursДокумент7 страницA Study On The Reasons For Transgender To Become EntrepreneursIAEME PublicationОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Analyse The User Predilection On Gpay and Phonepe For Digital TransactionsДокумент7 страницAnalyse The User Predilection On Gpay and Phonepe For Digital TransactionsIAEME PublicationОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Impact of Emotional Intelligence On Human Resource Management Practices Among The Remote Working It EmployeesДокумент10 страницImpact of Emotional Intelligence On Human Resource Management Practices Among The Remote Working It EmployeesIAEME PublicationОценок пока нет
- Voice Based Atm For Visually Impaired Using ArduinoДокумент7 страницVoice Based Atm For Visually Impaired Using ArduinoIAEME PublicationОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Modeling and Analysis of Surface Roughness and White Later Thickness in Wire-Electric Discharge Turning Process Through Response Surface MethodologyДокумент14 страницModeling and Analysis of Surface Roughness and White Later Thickness in Wire-Electric Discharge Turning Process Through Response Surface MethodologyIAEME PublicationОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Study On Talent Management and Its Impact On Employee Retention in Selected It Organizations in ChennaiДокумент16 страницA Study On Talent Management and Its Impact On Employee Retention in Selected It Organizations in ChennaiIAEME PublicationОценок пока нет
- A Proficient Minimum-Routine Reliable Recovery Line Accumulation Scheme For Non-Deterministic Mobile Distributed FrameworksДокумент10 страницA Proficient Minimum-Routine Reliable Recovery Line Accumulation Scheme For Non-Deterministic Mobile Distributed FrameworksIAEME PublicationОценок пока нет
- Gandhi On Non-Violent PoliceДокумент8 страницGandhi On Non-Violent PoliceIAEME PublicationОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Influence of Talent Management Practices On Organizational Performance A Study With Reference To It Sector in ChennaiДокумент16 страницInfluence of Talent Management Practices On Organizational Performance A Study With Reference To It Sector in ChennaiIAEME PublicationОценок пока нет
- A Study On The Impact of Organizational Culture On The Effectiveness of Performance Management Systems in Healthcare Organizations at ThanjavurДокумент7 страницA Study On The Impact of Organizational Culture On The Effectiveness of Performance Management Systems in Healthcare Organizations at ThanjavurIAEME PublicationОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Visualising Aging Parents & Their Close Carers Life Journey in Aging EconomyДокумент4 страницыVisualising Aging Parents & Their Close Carers Life Journey in Aging EconomyIAEME PublicationОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Attrition in The It Industry During Covid-19 Pandemic: Linking Emotional Intelligence and Talent Management ProcessesДокумент15 страницAttrition in The It Industry During Covid-19 Pandemic: Linking Emotional Intelligence and Talent Management ProcessesIAEME PublicationОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- A Study of Various Types of Loans of Selected Public and Private Sector Banks With Reference To Npa in State HaryanaДокумент9 страницA Study of Various Types of Loans of Selected Public and Private Sector Banks With Reference To Npa in State HaryanaIAEME PublicationОценок пока нет
- EXPERIMENTAL STUDY OF MECHANICAL AND TRIBOLOGICAL RELATION OF NYLON/BaSO4 POLYMER COMPOSITESДокумент9 страницEXPERIMENTAL STUDY OF MECHANICAL AND TRIBOLOGICAL RELATION OF NYLON/BaSO4 POLYMER COMPOSITESIAEME PublicationОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Role of Social Entrepreneurship in Rural Development of India - Problems and ChallengesДокумент18 страницRole of Social Entrepreneurship in Rural Development of India - Problems and ChallengesIAEME PublicationОценок пока нет
- Application of Frugal Approach For Productivity Improvement - A Case Study of Mahindra and Mahindra LTDДокумент19 страницApplication of Frugal Approach For Productivity Improvement - A Case Study of Mahindra and Mahindra LTDIAEME PublicationОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- A Multiple - Channel Queuing Models On Fuzzy EnvironmentДокумент13 страницA Multiple - Channel Queuing Models On Fuzzy EnvironmentIAEME PublicationОценок пока нет
- Analysis of Fuzzy Inference System Based Interline Power Flow Controller For Power System With Wind Energy Conversion System During Faulted ConditionsДокумент13 страницAnalysis of Fuzzy Inference System Based Interline Power Flow Controller For Power System With Wind Energy Conversion System During Faulted ConditionsIAEME PublicationОценок пока нет
- Optimal Reconfiguration of Power Distribution Radial Network Using Hybrid Meta-Heuristic AlgorithmsДокумент13 страницOptimal Reconfiguration of Power Distribution Radial Network Using Hybrid Meta-Heuristic AlgorithmsIAEME PublicationОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Various Fuzzy Numbers and Their Various Ranking ApproachesДокумент10 страницVarious Fuzzy Numbers and Their Various Ranking ApproachesIAEME PublicationОценок пока нет
- Dealing With Recurrent Terminates in Orchestrated Reliable Recovery Line Accumulation Algorithms For Faulttolerant Mobile Distributed SystemsДокумент8 страницDealing With Recurrent Terminates in Orchestrated Reliable Recovery Line Accumulation Algorithms For Faulttolerant Mobile Distributed SystemsIAEME PublicationОценок пока нет
- Prediction of Average Total Project Duration Using Artificial Neural Networks, Fuzzy Logic, and Regression ModelsДокумент13 страницPrediction of Average Total Project Duration Using Artificial Neural Networks, Fuzzy Logic, and Regression ModelsIAEME PublicationОценок пока нет
- A Review of Particle Swarm Optimization (Pso) AlgorithmДокумент26 страницA Review of Particle Swarm Optimization (Pso) AlgorithmIAEME PublicationОценок пока нет
- Financial Literacy On Investment Performance: The Mediating Effect of Big-Five Personality Traits ModelДокумент9 страницFinancial Literacy On Investment Performance: The Mediating Effect of Big-Five Personality Traits ModelIAEME PublicationОценок пока нет
- Knowledge Self-Efficacy and Research Collaboration Towards Knowledge Sharing: The Moderating Effect of Employee CommitmentДокумент8 страницKnowledge Self-Efficacy and Research Collaboration Towards Knowledge Sharing: The Moderating Effect of Employee CommitmentIAEME PublicationОценок пока нет
- Moderating Effect of Job Satisfaction On Turnover Intention and Stress Burnout Among Employees in The Information Technology SectorДокумент7 страницModerating Effect of Job Satisfaction On Turnover Intention and Stress Burnout Among Employees in The Information Technology SectorIAEME PublicationОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Quality of Work-Life On Employee Retention and Job Satisfaction: The Moderating Role of Job PerformanceДокумент7 страницQuality of Work-Life On Employee Retention and Job Satisfaction: The Moderating Role of Job PerformanceIAEME PublicationОценок пока нет
- Analysis On Machine Cell Recognition and Detaching From Neural SystemsДокумент9 страницAnalysis On Machine Cell Recognition and Detaching From Neural SystemsIAEME PublicationОценок пока нет
- MFD16I003 FinalДокумент16 страницMFD16I003 FinalAditya KumarОценок пока нет
- Adhesive Film & TapeДокумент6 страницAdhesive Film & TapeJothi Vel MuruganОценок пока нет
- Acc 106 Account ReceivablesДокумент40 страницAcc 106 Account ReceivablesAmirah NordinОценок пока нет
- AT10 Meat Tech 1Документ20 страницAT10 Meat Tech 1Reubal Jr Orquin Reynaldo100% (1)
- Matokeo CBДокумент4 страницыMatokeo CBHubert MubofuОценок пока нет
- The Attachment To Woman's Virtue in Abdulrazak Gurnah's Desertion (2005)Документ7 страницThe Attachment To Woman's Virtue in Abdulrazak Gurnah's Desertion (2005)IJELS Research JournalОценок пока нет
- Asme b16.3 (1998) Malleable Iron Threaded FittingsДокумент30 страницAsme b16.3 (1998) Malleable Iron Threaded FittingsMarcos RosenbergОценок пока нет
- Corregidor Title DefenseДокумент16 страницCorregidor Title DefenseJaydee ColadillaОценок пока нет
- Indian Traditional Musical InstrumentsДокумент3 страницыIndian Traditional Musical InstrumentsPiriya94Оценок пока нет
- Journal Articles: Types of JournalsДокумент4 страницыJournal Articles: Types of JournalsOtieno SteveОценок пока нет
- E9 Đề khảo sát Trưng Vương 2022 ex No 1Документ4 страницыE9 Đề khảo sát Trưng Vương 2022 ex No 1Minh TiếnОценок пока нет
- A Sample Script For Public SpeakingДокумент2 страницыA Sample Script For Public Speakingalmasodi100% (2)
- TV Antenna Tower CollapseДокумент4 страницыTV Antenna Tower CollapseImdaad ChuubbОценок пока нет
- Old Highland Park Baptist Church E01Документ74 страницыOld Highland Park Baptist Church E01Lawrence Garner100% (2)
- APRStt Implementation Notes PDFДокумент36 страницAPRStt Implementation Notes PDFCT2IWWОценок пока нет
- SetupДокумент4 страницыSetupRsam SamrОценок пока нет
- Eu Clinical TrialДокумент4 страницыEu Clinical TrialAquaОценок пока нет
- DISTRICT CENSUS HANDBOOK North GoaДокумент190 страницDISTRICT CENSUS HANDBOOK North Goants1020Оценок пока нет
- Choosing An Effective Visual ToolДокумент9 страницChoosing An Effective Visual ToolAdil Bin KhalidОценок пока нет
- 3.2.1 The Role of Market Research and Methods UsedДокумент42 страницы3.2.1 The Role of Market Research and Methods Usedsana jaleelОценок пока нет
- Javascript NotesДокумент5 страницJavascript NotesRajashekar PrasadОценок пока нет
- Automated Facilities Layout Past Present and FutureДокумент19 страницAutomated Facilities Layout Past Present and FutureJose Luis Diaz BetancourtОценок пока нет
- Best of The Photo DetectiveДокумент55 страницBest of The Photo DetectiveSazeed Hossain100% (3)
- Sample Valuation ReportДокумент15 страницSample Valuation Reportayush singlaОценок пока нет
- Bofa Turkish Banks-Back On The RadarДокумент15 страницBofa Turkish Banks-Back On The RadarexperhtmОценок пока нет
- Silapathikaram 3Документ37 страницSilapathikaram 3gavinilaaОценок пока нет
- 8. Nguyễn Tất Thành- Kon TumДокумент17 страниц8. Nguyễn Tất Thành- Kon TumK60 TRẦN MINH QUANGОценок пока нет
- Grade 10 Module 1 Performing Roughing in Activities For Communication and DistributДокумент26 страницGrade 10 Module 1 Performing Roughing in Activities For Communication and DistributNelshane JohnОценок пока нет
- Ch04Exp PDFДокумент17 страницCh04Exp PDFConstantin PopescuОценок пока нет
- Npad PGP2017-19Документ3 страницыNpad PGP2017-19Nikhil BhattОценок пока нет
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (393)