Вам также может понравиться
- Transcultural Nursing TheoryДокумент17 страницTranscultural Nursing TheoryJR Rolf Neuqelet100% (1)
- Transcultural Nursing TheoryДокумент16 страницTranscultural Nursing TheoryJR Rolf NeuqeletОценок пока нет
- Presentation Transcultural NursingДокумент23 страницыPresentation Transcultural NursingHazel Eñga Tiam Wat100% (2)
- I. Madeleine LeiningerДокумент5 страницI. Madeleine LeiningerBSN-2F Neutral Axis SiazonОценок пока нет
- Compilation TFNДокумент65 страницCompilation TFNEliakim III InsongОценок пока нет
- Grand Theories: THEORY: Transcultural NursingДокумент15 страницGrand Theories: THEORY: Transcultural NursingMiden AlbanoОценок пока нет
- LeiningerДокумент36 страницLeiningerAshley EmperadorОценок пока нет
- Madeleine LeiningerДокумент4 страницыMadeleine LeiningergandhyvoltronОценок пока нет
- Biography of Madeleine Leininger: Leininger's Transcultural Nursing TheoryДокумент7 страницBiography of Madeleine Leininger: Leininger's Transcultural Nursing Theorykristel ann matelaОценок пока нет
- TRanscultural Nursing CritiqueДокумент3 страницыTRanscultural Nursing CritiquekyreОценок пока нет
- Week 6Документ23 страницыWeek 6Rhesie Joyce AguilarОценок пока нет
- (Consumers) Working Together To Identify, Plan, Implement, and Evaluate EachДокумент3 страницы(Consumers) Working Together To Identify, Plan, Implement, and Evaluate EachJarLo GranadaОценок пока нет
- ch15 MADELEINE LEININGERpdfДокумент8 страницch15 MADELEINE LEININGERpdfnirvangel13Оценок пока нет
- TCN 2Документ29 страницTCN 2Glory Anne Joy WillyОценок пока нет
- Trancultural Nursing: EssayДокумент6 страницTrancultural Nursing: EssayJoko Tri WahyudiОценок пока нет
- Trancu NotesДокумент4 страницыTrancu NotesCharme Jean RaygonОценок пока нет
- Madeleine LeiningerДокумент38 страницMadeleine LeiningerCharina AubreyОценок пока нет
- Madeleine Leininger Transcultural NursingДокумент5 страницMadeleine Leininger Transcultural Nursingteabagman100% (1)
- Decent Work Employment and Transcultural Nursing NCM 120: Ma. Esperanza E. Reavon, Man, RNДокумент64 страницыDecent Work Employment and Transcultural Nursing NCM 120: Ma. Esperanza E. Reavon, Man, RNMa. Esperanza C. Eijansantos-Reavon100% (1)
- Nursing Theories of Adbellah, Travelbee, Leininger and ParseДокумент92 страницыNursing Theories of Adbellah, Travelbee, Leininger and ParseYo MamaОценок пока нет
- Back UpДокумент49 страницBack UpJoem Cerio PerinaОценок пока нет
- Transcultrural Nursing PDFДокумент6 страницTranscultrural Nursing PDFSarithaRajeshОценок пока нет
- Madeline Linger TCNT AssignmentДокумент41 страницаMadeline Linger TCNT Assignmentweldish1314Оценок пока нет
- TFN ReviewerДокумент16 страницTFN ReviewerLunaОценок пока нет
- Culture Care Theory: By: Jennah Ercy S. de Leon, RNДокумент18 страницCulture Care Theory: By: Jennah Ercy S. de Leon, RNmaria cristina lugayОценок пока нет
- Grand Nursing - Transcultural Nursing TheoryДокумент8 страницGrand Nursing - Transcultural Nursing TheoryJhunmae KindipanОценок пока нет
- Nursing Theories GuideДокумент15 страницNursing Theories Guideapi-532304340Оценок пока нет
- Dokumen Dari UlfaДокумент6 страницDokumen Dari UlfaAnnisa UlfaОценок пока нет
- Konsep Teori Transkultural Nursing LeninggerДокумент26 страницKonsep Teori Transkultural Nursing LeninggerEdo WilsonОценок пока нет
- Chapter 9 Nursing Celebrates Cultural DiversityДокумент12 страницChapter 9 Nursing Celebrates Cultural DiversityDon DxОценок пока нет
- Leininger2 - Culture Care Universality & DiversityДокумент32 страницыLeininger2 - Culture Care Universality & Diversitymao ayunan (misaki minna ayunan)Оценок пока нет
- Analisis Teori Madeleine LeiningerДокумент2 страницыAnalisis Teori Madeleine LeiningerKing DonОценок пока нет
- TransculturalДокумент13 страницTransculturalDONALDОценок пока нет
- Holistic Care and Transcultural NursingДокумент26 страницHolistic Care and Transcultural NursingferaОценок пока нет
- Trans Cultural NursingДокумент29 страницTrans Cultural NursingJude Bello-Alvear100% (1)
- 11 TFN - Transcultural-Nursing-Concepts-theories-and-practicesДокумент29 страниц11 TFN - Transcultural-Nursing-Concepts-theories-and-practicesLalaineОценок пока нет
- Bahan LTMДокумент23 страницыBahan LTMEpi SapitriОценок пока нет
- Madeleine LeiningerДокумент2 страницыMadeleine Leiningerdumbwaste528Оценок пока нет
- Major Concepts of The Transcultural Nursing TheoryДокумент5 страницMajor Concepts of The Transcultural Nursing TheoryASTRA FAYE QUEENA DELENAОценок пока нет
- TFN DS 16 - LeiningerДокумент31 страницаTFN DS 16 - LeiningerCatherine Martinez AvilaОценок пока нет
- Madeline Leininger's Transculural NursingДокумент23 страницыMadeline Leininger's Transculural NursingMae lea AndoloyОценок пока нет
- 1.seminar Transcultural Nursing-1Документ29 страниц1.seminar Transcultural Nursing-1Reshma rsr100% (3)
- Transcultural NursingДокумент32 страницыTranscultural Nursingnovi100% (2)
- Reviewer 19 MADELINE LEININGERДокумент3 страницыReviewer 19 MADELINE LEININGERClaireОценок пока нет
- Transcultural NSG HX Theory Cultural AssstДокумент73 страницыTranscultural NSG HX Theory Cultural AssstJorie RocoОценок пока нет
- Transcultural Nursing Nur324Документ18 страницTranscultural Nursing Nur324lidyaОценок пока нет
- Why Is Cultural Knowledge Important To Nurses?: Cultural Competency in NursingДокумент4 страницыWhy Is Cultural Knowledge Important To Nurses?: Cultural Competency in NursingFitriia SariiОценок пока нет
- Culture Care TheoryДокумент24 страницыCulture Care Theorydileepkumar.duhs4817100% (6)
- 2185 4494 1 SM PDFДокумент32 страницы2185 4494 1 SM PDFUlfahОценок пока нет
- Leininger's Culture Care Theory - Nursing TheoryДокумент4 страницыLeininger's Culture Care Theory - Nursing TheoryLolaОценок пока нет
- Cultural Diversity in Nursing PracticeДокумент3 страницыCultural Diversity in Nursing PracticeEli Xma100% (2)
- Bachelor of Science in Nursing: Bioethics/Health Care EthicsДокумент10 страницBachelor of Science in Nursing: Bioethics/Health Care EthicsDenise FranciscoОценок пока нет
- Madeleine LeiningerДокумент20 страницMadeleine LeiningerTin LopezОценок пока нет
- FWD 2 Copies by 5 TH AprilДокумент9 страницFWD 2 Copies by 5 TH Aprilhoodyfoody09Оценок пока нет
- At LTC N Theories Models 1Документ35 страницAt LTC N Theories Models 1Darin BransonОценок пока нет
- Madeleine LeiningerДокумент21 страницаMadeleine LeiningerMikz JocomОценок пока нет
- LeiningerДокумент5 страницLeiningerellesor07100% (1)
- A Research Output On Transcultural Nursing and Globalization of Health Care and The Different Theoretical Perspectives of Transcultural NursingДокумент24 страницыA Research Output On Transcultural Nursing and Globalization of Health Care and The Different Theoretical Perspectives of Transcultural NursingOrlino PeterОценок пока нет
- Cape MCQ 08-13Документ51 страницаCape MCQ 08-13brown_chocolate87643Оценок пока нет
- PBL2Документ12 страницPBL2brown_chocolate87643Оценок пока нет
- Normocytic Anemia'sДокумент14 страницNormocytic Anemia'sbrown_chocolate87643Оценок пока нет
- Phil Must Be Asked For Permission To Sample Blood For A HCV and HIV Test. If He Refuses Then It Must Be Assumed He Is A Carrier of The VirusДокумент3 страницыPhil Must Be Asked For Permission To Sample Blood For A HCV and HIV Test. If He Refuses Then It Must Be Assumed He Is A Carrier of The Virusbrown_chocolate87643Оценок пока нет
- POM Class 1 For MD7-2Документ2 страницыPOM Class 1 For MD7-2brown_chocolate87643Оценок пока нет
- Nimesulide Patients Still Exposed To A Risk of Severe HepatitisДокумент2 страницыNimesulide Patients Still Exposed To A Risk of Severe Hepatitisbrown_chocolate87643Оценок пока нет
- Real Comm Studies IA-2Документ7 страницReal Comm Studies IA-2brown_chocolate87643Оценок пока нет
- Ghouls Bhowling Alley Kiss of Death Wiked Cricket Grab Bag and More!!!Документ2 страницыGhouls Bhowling Alley Kiss of Death Wiked Cricket Grab Bag and More!!!brown_chocolate87643Оценок пока нет
- Summer Course 2014 FlyerДокумент1 страницаSummer Course 2014 Flyerbrown_chocolate87643Оценок пока нет
- Question 3 Micro B-2Документ3 страницыQuestion 3 Micro B-2brown_chocolate87643Оценок пока нет
- AAIMS INVITATION - 4th Anniversary LectureДокумент1 страницаAAIMS INVITATION - 4th Anniversary Lecturebrown_chocolate87643Оценок пока нет
- Communication Skills 11 ExaminationДокумент8 страницCommunication Skills 11 Examinationbrown_chocolate87643Оценок пока нет
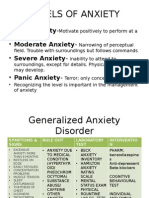
- Levels of Anxiety: - Mild Anxiety - Moderate Anxiety - Severe Anxiety - Panic AnxietyДокумент4 страницыLevels of Anxiety: - Mild Anxiety - Moderate Anxiety - Severe Anxiety - Panic Anxietybrown_chocolate87643Оценок пока нет
- Sports DayДокумент4 страницыSports Daybrown_chocolate87643Оценок пока нет
- Anemias: Table Showing Types of Anemias and Causes Reticulocyte Count Microcytic Normocytic Macrocytic LOWДокумент4 страницыAnemias: Table Showing Types of Anemias and Causes Reticulocyte Count Microcytic Normocytic Macrocytic LOWbrown_chocolate87643Оценок пока нет
- Case 34Документ10 страницCase 34brown_chocolate87643Оценок пока нет
- Mass in Epigastrium-2Документ37 страницMass in Epigastrium-2brown_chocolate87643100% (1)
- Signed Off - Personality Developent11 - q1 - m3 - Coping With Stress in Middle and Late Adolescence and The Powers of The Mind - v3 PDFДокумент29 страницSigned Off - Personality Developent11 - q1 - m3 - Coping With Stress in Middle and Late Adolescence and The Powers of The Mind - v3 PDFRaniel John Avila Sampiano80% (5)
- Why Study HistoryДокумент1 страницаWhy Study Historyregine_liОценок пока нет
- Video Classroom Observation FormДокумент4 страницыVideo Classroom Observation FormPhil ChappellОценок пока нет
- Chitra NakshatraДокумент12 страницChitra NakshatraSri KayОценок пока нет
- Tpa 1Документ11 страницTpa 1api-501103450Оценок пока нет
- Wonderlic Scholastic Level Exam Sample Questions: AnswersДокумент1 страницаWonderlic Scholastic Level Exam Sample Questions: AnswersElize FontesОценок пока нет
- School Nursing SyllabusДокумент4 страницыSchool Nursing SyllabusFirenze Fil100% (1)
- What Is Political EconomyДокумент10 страницWhat Is Political EconomyayulatifahОценок пока нет
- MS401L16 Ready and Resilient Program SRДокумент5 страницMS401L16 Ready and Resilient Program SRAlex LogvinovskyОценок пока нет
- FreeLandformsBulletinBoardPostersandMatchingActivity PDFДокумент28 страницFreeLandformsBulletinBoardPostersandMatchingActivity PDFDharani JagadeeshОценок пока нет
- Mercer TalentSIMДокумент3 страницыMercer TalentSIMJelenaMiloševićОценок пока нет
- A Study On Customer Satisfaction Towards " Asian Paints" (With Reference To Hightech Paint Shopee, Adoni)Документ7 страницA Study On Customer Satisfaction Towards " Asian Paints" (With Reference To Hightech Paint Shopee, Adoni)RameshОценок пока нет
- 10-15'-ĐỀ CHẴNДокумент2 страницы10-15'-ĐỀ CHẴNSơn HoàngОценок пока нет
- Ocean Breeze Invitational Girls Heat SheetsДокумент33 страницыOcean Breeze Invitational Girls Heat SheetsAshley TysiacОценок пока нет
- Pengajian Malaysia AssignmentДокумент11 страницPengajian Malaysia AssignmentNorra Zuckerberg Belkin100% (1)
- International Conservation Project Funders: Institution Award/Scholarship Description Award Amount WebsiteДокумент22 страницыInternational Conservation Project Funders: Institution Award/Scholarship Description Award Amount WebsitenicdonatiОценок пока нет
- COT 1 Plate Boundaries Science 10Документ6 страницCOT 1 Plate Boundaries Science 10Christy Rose VelascoОценок пока нет
- Assignment 01 Pyc4805Документ2 страницыAssignment 01 Pyc4805nancyОценок пока нет
- Comparing Numbers (2021 - 06 - 19 01 - 35 - 12 UTC) (2021 - 08 - 06 04 - 51 - 25 UTC)Документ3 страницыComparing Numbers (2021 - 06 - 19 01 - 35 - 12 UTC) (2021 - 08 - 06 04 - 51 - 25 UTC)ALLinOne BlogОценок пока нет
- 2021 Mechatronics CurriculumДокумент5 страниц2021 Mechatronics CurriculumGalaxy AtomОценок пока нет
- Department of Education: National Capital Region Schools Division Office of Quezon City Quezon City High SchoolДокумент3 страницыDepartment of Education: National Capital Region Schools Division Office of Quezon City Quezon City High SchoolJonathanEncomiendaОценок пока нет
- EF3e Adv Quicktest 05 OverlayДокумент1 страницаEF3e Adv Quicktest 05 OverlayАрина АхметжановаОценок пока нет
- Dhaval CVДокумент2 страницыDhaval CVPurva PrajapatiОценок пока нет
- Why Should A Researcher Conduct Literature ReviewДокумент7 страницWhy Should A Researcher Conduct Literature Reviewc5p4r60cОценок пока нет
- Oral Language, Stance, and Behavior Different Communication SituationsДокумент82 страницыOral Language, Stance, and Behavior Different Communication SituationsPRINCESS DOMINIQUE ALBERTOОценок пока нет
- Synopsis OSCEДокумент5 страницSynopsis OSCEPrasann RoyОценок пока нет
- Wise SpendingДокумент5 страницWise SpendingFatiyarrОценок пока нет
- Bartle Elements of Integration and Lebesgue MeasureДокумент20 страницBartle Elements of Integration and Lebesgue MeasureAlejandro FandiñoОценок пока нет
- Demo June 5Документ10 страницDemo June 5Mae Ann Carreon TrapalОценок пока нет
- Year 4 Cefr Writing LPДокумент2 страницыYear 4 Cefr Writing LPKannan Thiagarajan100% (1)