Вам также может понравиться
- Diagnostic Limitations of Cephalometrics in OrthodonticsДокумент6 страницDiagnostic Limitations of Cephalometrics in OrthodonticsDevata RaviОценок пока нет
- Fixed Orthodontic Appliances: A Practical GuideОт EverandFixed Orthodontic Appliances: A Practical GuideРейтинг: 1 из 5 звезд1/5 (1)
- Principles of The Alexander DisciplineДокумент5 страницPrinciples of The Alexander DisciplineSarah Fauzia SiregarОценок пока нет
- Class III TTT OptionsДокумент9 страницClass III TTT OptionsMADAОценок пока нет
- WittsДокумент39 страницWittsAya ElsayedОценок пока нет
- A Review of Root Resorption in Orthodontics PDFДокумент5 страницA Review of Root Resorption in Orthodontics PDFRahulLife'sОценок пока нет
- Transpositions: C H A P T e RДокумент8 страницTranspositions: C H A P T e Rjohnmax100% (2)
- Artificial Intelligence in Orthodontics A Review ArticleДокумент5 страницArtificial Intelligence in Orthodontics A Review ArticleInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- The Orthodontics Effective RoleДокумент31 страницаThe Orthodontics Effective RoleHamza BelhajОценок пока нет
- Expansion in The Absence of Crossbite - Rationale and ProtocolДокумент12 страницExpansion in The Absence of Crossbite - Rationale and Protocoljeyran efarsani100% (1)
- Behavior OrthoДокумент96 страницBehavior OrthoarshabharataОценок пока нет
- Journal Club1 / Orthodontic Courses by Indian Dental AcademyДокумент19 страницJournal Club1 / Orthodontic Courses by Indian Dental Academyindian dental academyОценок пока нет
- A Talon Cusp PDFДокумент3 страницыA Talon Cusp PDFNajeeb UllahОценок пока нет
- Ricketts TriadДокумент23 страницыRicketts TriadSonu RajuОценок пока нет
- Alexander DisiplineДокумент17 страницAlexander DisiplineAshish SharmaОценок пока нет
- Mechanics in OccДокумент29 страницMechanics in OccDrAla MohamedОценок пока нет
- MANAGEMENT OF VERTICAL MAXILLARY EXCESS WWWДокумент24 страницыMANAGEMENT OF VERTICAL MAXILLARY EXCESS WWWsweetieОценок пока нет
- Methods of Correction of Unilateral Posterior CrossbiteДокумент36 страницMethods of Correction of Unilateral Posterior CrossbiteSwathiLingannagariОценок пока нет
- Bomechancs in OrthodotnicsДокумент74 страницыBomechancs in OrthodotnicsheycoolalexОценок пока нет
- Intrusion Arches ShinuДокумент66 страницIntrusion Arches ShinuYuvashreeОценок пока нет
- Beta Angle 2003Документ6 страницBeta Angle 2003surendra334Оценок пока нет
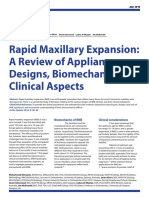
- Rapid Maxillary Expansion - Appliance Designs, Biomechanics and Clinical Aspects PDFДокумент5 страницRapid Maxillary Expansion - Appliance Designs, Biomechanics and Clinical Aspects PDFLanaОценок пока нет
- Abo Objective Grading System PDFДокумент11 страницAbo Objective Grading System PDFNasira Adnan100% (1)
- Orthodontic Management of A Maxillary Midline Diastema Using Beggs Mechanics Case ReportДокумент3 страницыOrthodontic Management of A Maxillary Midline Diastema Using Beggs Mechanics Case ReportEditor IJTSRDОценок пока нет
- Pain ManagementДокумент44 страницыPain ManagementSaherish FarhanОценок пока нет
- Self Ligating BracketsДокумент5 страницSelf Ligating BracketsSreenivasa Krishna ChaitanyaОценок пока нет
- Intrusion MechanicsДокумент31 страницаIntrusion Mechanicsaa bbОценок пока нет
- Ceph HandoutДокумент18 страницCeph Handoutwaheguru13he13Оценок пока нет
- Cellular, Molecular, and Tissue-Level Reactions To Orthodontic ForceДокумент32 страницыCellular, Molecular, and Tissue-Level Reactions To Orthodontic Forcecarlina_the_bestОценок пока нет
- Retention and Relapse SeminarДокумент51 страницаRetention and Relapse SeminarShipra SehgalОценок пока нет
- History of OrthodonticsДокумент3 страницыHistory of OrthodonticsJuliusRanteОценок пока нет
- A Dilemma in Orthodontics Extractions in Borderline CasesДокумент4 страницыA Dilemma in Orthodontics Extractions in Borderline CasesOsama MohamedОценок пока нет
- Lillian B. MVSS, N.i) .S., XS.," kRORA, ILL: (1786) U-As OneДокумент21 страницаLillian B. MVSS, N.i) .S., XS.," kRORA, ILL: (1786) U-As OneDiana Paola FontechaОценок пока нет
- Risk and Limitations of Orthodontic TreatmentДокумент41 страницаRisk and Limitations of Orthodontic TreatmentAjay ChhetriОценок пока нет
- Current Topics and Controversies Presented by DR Anthony GianellyДокумент2 страницыCurrent Topics and Controversies Presented by DR Anthony GianellyIvanna H. A.Оценок пока нет
- Activator HeadgearДокумент9 страницActivator HeadgearThendral DevanathanОценок пока нет
- Cone Beam Tomography in Orthodontics PDFДокумент8 страницCone Beam Tomography in Orthodontics PDFdruzair007Оценок пока нет
- Smile Analysis: A Review Part IIДокумент4 страницыSmile Analysis: A Review Part IIGustavoAndresGarciaОценок пока нет
- Eccentric RelationДокумент10 страницEccentric RelationKiana TediОценок пока нет
- Moving The TeethДокумент117 страницMoving The TeethThirunavukkarasu Srinivasan100% (2)
- Biomechanics of TorqueДокумент8 страницBiomechanics of TorquehemaadriОценок пока нет
- Functional Appliances: Click To Edit Master Subtitle Style Dr. Rashid MahmoodДокумент150 страницFunctional Appliances: Click To Edit Master Subtitle Style Dr. Rashid MahmoodZawara MariamОценок пока нет
- Potential and Limitations of Orthodontic Biomechanics RecognizingДокумент9 страницPotential and Limitations of Orthodontic Biomechanics RecognizingLisbethОценок пока нет
- Differential Diagnostic Analysis System: Clinicians' CornerДокумент8 страницDifferential Diagnostic Analysis System: Clinicians' CornerSawita KumariОценок пока нет
- Bi-Helix Space Opening Spring For Lingual OrthodonДокумент3 страницыBi-Helix Space Opening Spring For Lingual OrthodonYessenya FlxОценок пока нет
- Diagnosis and Treatment PlanningДокумент93 страницыDiagnosis and Treatment PlanningVikkii VeerakumarОценок пока нет
- Early Treatment of Vertical Skeletal DysplasiaДокумент11 страницEarly Treatment of Vertical Skeletal Dysplasiagilberto69Оценок пока нет
- Bowden1978 Theoretical Considerations of Headgear Therapy 2Документ10 страницBowden1978 Theoretical Considerations of Headgear Therapy 2solodont1Оценок пока нет
- Inhouse Aligners-A Review ArticleДокумент6 страницInhouse Aligners-A Review ArticleInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Vari-Simplex DisciplineДокумент60 страницVari-Simplex DisciplineDrGurinder Kanwar100% (1)
- Comparison Between Surgically-Assisted Rapid Palatal Expansion (Sarpe) and Miniscrew-Assisted Rapid Palatal Expansion (Marpe) A Systematic ReviewДокумент28 страницComparison Between Surgically-Assisted Rapid Palatal Expansion (Sarpe) and Miniscrew-Assisted Rapid Palatal Expansion (Marpe) A Systematic Reviewaa bbОценок пока нет
- Tweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisДокумент56 страницTweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisAnonymous 1uVifBp6100% (1)
- Equilibrium Theory of Tooth Position IIДокумент12 страницEquilibrium Theory of Tooth Position IILIZETH NATHALIA TOLOZA OCHOAОценок пока нет
- A Century of The Edgewise Appliance11Документ11 страницA Century of The Edgewise Appliance11Jingxuan LuoОценок пока нет
- Anterior and Canine RetractionДокумент10 страницAnterior and Canine RetractionLisbethОценок пока нет
- CLASSIC ARTICLE Clinical Measurement and EvaluationДокумент5 страницCLASSIC ARTICLE Clinical Measurement and EvaluationJesusCordoba100% (2)
- Boltons AnalysisДокумент18 страницBoltons AnalysisAchint JunejaОценок пока нет
- A Method of Cephalometric Evaluation Mcnamara 1984Документ21 страницаA Method of Cephalometric Evaluation Mcnamara 1984Gaurav Pratap SinghОценок пока нет
- 2.assessment of Dental Crowding in Mandibular Anterior Region by Three Different MethodsДокумент3 страницы2.assessment of Dental Crowding in Mandibular Anterior Region by Three Different MethodsJennifer Abella Brown0% (1)
- Antegonial NotchДокумент3 страницыAntegonial NotchpveginaduОценок пока нет
- Butler's Field TheoryДокумент5 страницButler's Field Theorypveginadu100% (1)
- Genetic Influence On Class II Div 2Документ12 страницGenetic Influence On Class II Div 2pveginaduОценок пока нет
- The Role of The Golden Proportion in The Evaluation of Facial EstheticsДокумент8 страницThe Role of The Golden Proportion in The Evaluation of Facial EstheticspveginaduОценок пока нет
- Angles Line of OcclusionДокумент9 страницAngles Line of OcclusionpveginaduОценок пока нет
- Looping Case StudyДокумент9 страницLooping Case StudyMukesh Kumar SinghОценок пока нет
- Network LayerДокумент134 страницыNetwork Layershivang pandeyОценок пока нет
- Long Report DsДокумент21 страницаLong Report DsNabilah AzizОценок пока нет
- Statistics and Probability Yong Hwa M. Jeong Grade 11 STEM-B Quarter 4 - Module 1: Test of HypothesisДокумент22 страницыStatistics and Probability Yong Hwa M. Jeong Grade 11 STEM-B Quarter 4 - Module 1: Test of HypothesisSarahmae MeñozaОценок пока нет
- Cse 205: Digital Logic Design: Dr. Tanzima Hashem Assistant Professor Cse, BuetДокумент55 страницCse 205: Digital Logic Design: Dr. Tanzima Hashem Assistant Professor Cse, BuetShakib AhmedОценок пока нет
- 15-381 Spring 2007 Assignment 6: LearningДокумент14 страниц15-381 Spring 2007 Assignment 6: LearningsandeepanОценок пока нет
- 3rd PrepДокумент61 страница3rd Prepmohamed faroukОценок пока нет
- Cambridge IGCSE: MATHEMATICS 0580/33Документ20 страницCambridge IGCSE: MATHEMATICS 0580/33Hussain JassimОценок пока нет
- Uplifting The Skills in Solving Word Problems Using Selected Literacy Strategies For Grade 6 MathematicsДокумент18 страницUplifting The Skills in Solving Word Problems Using Selected Literacy Strategies For Grade 6 Mathematicscherkarlo100% (1)
- 19 Tips For Nested IF FormulasДокумент15 страниц19 Tips For Nested IF FormulasGodfrey KakalaОценок пока нет
- Micro GridДокумент5 страницMicro GridArif IbrahimОценок пока нет
- DLP Grade 7-10 Matter With LinkДокумент104 страницыDLP Grade 7-10 Matter With LinklovelyОценок пока нет
- GNL 05Документ4 страницыGNL 05Mauricio Bustamante HuaquipaОценок пока нет
- Lab 6 DFT and FFTДокумент16 страницLab 6 DFT and FFTZia UllahОценок пока нет
- NMF 8.3 - Pupil BookДокумент256 страницNMF 8.3 - Pupil BookKhaled DaoudОценок пока нет
- Quant WS Oct 4Документ2 страницыQuant WS Oct 4Time DehradunОценок пока нет
- Lab Notebook Grading Rubric: Category Proficient (4-5) Developing (2-3) Basic (0-1)Документ1 страницаLab Notebook Grading Rubric: Category Proficient (4-5) Developing (2-3) Basic (0-1)Parizay ChОценок пока нет
- Multiplying DecimalsДокумент2 страницыMultiplying Decimalsapi-233663523Оценок пока нет
- Numerical Structural Analysis - O'Hara, Steven (SRG) PDFДокумент302 страницыNumerical Structural Analysis - O'Hara, Steven (SRG) PDFggsarne100% (6)
- Combine - Asynchronous Programming With SwiftДокумент7 страницCombine - Asynchronous Programming With SwiftSrecko JanicijevicОценок пока нет
- TriangleДокумент12 страницTriangleAulia Adytia PutriОценок пока нет
- PLSQL 4 3 PracticeДокумент2 страницыPLSQL 4 3 PracticeNurul Fadillah JannahОценок пока нет
- Pharm-D 2nd Scheme of StudiesДокумент11 страницPharm-D 2nd Scheme of StudiesEyssa MalikОценок пока нет
- ApmДокумент11 страницApmsreyoshiОценок пока нет
- Structural Design of BinsДокумент34 страницыStructural Design of Binsjayaraman3Оценок пока нет
- Logistics Models: Question One (Exercise 6.1)Документ6 страницLogistics Models: Question One (Exercise 6.1)Olaolu JosephОценок пока нет
- Lec02 PDFДокумент6 страницLec02 PDFEka MarlyanaОценок пока нет
- Workshop 5 2D Axisymmetric Impact: Introduction To ANSYS Explicit STRДокумент20 страницWorkshop 5 2D Axisymmetric Impact: Introduction To ANSYS Explicit STRCosmin ConduracheОценок пока нет
- MCQ C Language ChapterwiseДокумент5 страницMCQ C Language Chapterwiseapi-267047853Оценок пока нет
- Mental Math Secrets - How To Be a Human CalculatorОт EverandMental Math Secrets - How To Be a Human CalculatorРейтинг: 5 из 5 звезд5/5 (3)
- A Mathematician's Lament: How School Cheats Us Out of Our Most Fascinating and Imaginative Art FormОт EverandA Mathematician's Lament: How School Cheats Us Out of Our Most Fascinating and Imaginative Art FormРейтинг: 5 из 5 звезд5/5 (5)
- Basic Math & Pre-Algebra Workbook For Dummies with Online PracticeОт EverandBasic Math & Pre-Algebra Workbook For Dummies with Online PracticeРейтинг: 4 из 5 звезд4/5 (2)
- Build a Mathematical Mind - Even If You Think You Can't Have One: Become a Pattern Detective. Boost Your Critical and Logical Thinking Skills.От EverandBuild a Mathematical Mind - Even If You Think You Can't Have One: Become a Pattern Detective. Boost Your Critical and Logical Thinking Skills.Рейтинг: 5 из 5 звезд5/5 (1)
- Quantum Physics: A Beginners Guide to How Quantum Physics Affects Everything around UsОт EverandQuantum Physics: A Beginners Guide to How Quantum Physics Affects Everything around UsРейтинг: 4.5 из 5 звезд4.5/5 (3)
- Fluent in 3 Months: How Anyone at Any Age Can Learn to Speak Any Language from Anywhere in the WorldОт EverandFluent in 3 Months: How Anyone at Any Age Can Learn to Speak Any Language from Anywhere in the WorldРейтинг: 3 из 5 звезд3/5 (80)
- Calculus Workbook For Dummies with Online PracticeОт EverandCalculus Workbook For Dummies with Online PracticeРейтинг: 3.5 из 5 звезд3.5/5 (8)
- Mathematical Mindsets: Unleashing Students' Potential through Creative Math, Inspiring Messages and Innovative TeachingОт EverandMathematical Mindsets: Unleashing Students' Potential through Creative Math, Inspiring Messages and Innovative TeachingРейтинг: 4.5 из 5 звезд4.5/5 (21)
- Mental Math: How to Develop a Mind for Numbers, Rapid Calculations and Creative Math Tricks (Including Special Speed Math for SAT, GMAT and GRE Students)От EverandMental Math: How to Develop a Mind for Numbers, Rapid Calculations and Creative Math Tricks (Including Special Speed Math for SAT, GMAT and GRE Students)Оценок пока нет
- Images of Mathematics Viewed Through Number, Algebra, and GeometryОт EverandImages of Mathematics Viewed Through Number, Algebra, and GeometryОценок пока нет
- ParaPro Assessment Preparation 2023-2024: Study Guide with 300 Practice Questions and Answers for the ETS Praxis Test (Paraprofessional Exam Prep)От EverandParaPro Assessment Preparation 2023-2024: Study Guide with 300 Practice Questions and Answers for the ETS Praxis Test (Paraprofessional Exam Prep)Оценок пока нет
- Math Workshop, Grade K: A Framework for Guided Math and Independent PracticeОт EverandMath Workshop, Grade K: A Framework for Guided Math and Independent PracticeРейтинг: 5 из 5 звезд5/5 (1)
- How Math Explains the World: A Guide to the Power of Numbers, from Car Repair to Modern PhysicsОт EverandHow Math Explains the World: A Guide to the Power of Numbers, from Car Repair to Modern PhysicsРейтинг: 3.5 из 5 звезд3.5/5 (9)
- A-level Maths Revision: Cheeky Revision ShortcutsОт EverandA-level Maths Revision: Cheeky Revision ShortcutsРейтинг: 3.5 из 5 звезд3.5/5 (8)
- A Guide to Success with Math: An Interactive Approach to Understanding and Teaching Orton Gillingham MathОт EverandA Guide to Success with Math: An Interactive Approach to Understanding and Teaching Orton Gillingham MathРейтинг: 5 из 5 звезд5/5 (1)