Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- SPAN CSP Volume 1Документ173 страницыSPAN CSP Volume 1samer alrawashdeh100% (1)
- Visitor T30 User's Manual - Rev07 PDFДокумент37 страницVisitor T30 User's Manual - Rev07 PDFDoaà SsalamОценок пока нет
- State Bank of IndiaДокумент1 страницаState Bank of IndiaKumar DasОценок пока нет
- Women's Empowerment Programs Experimental EvidenceДокумент27 страницWomen's Empowerment Programs Experimental EvidenceKumar DasОценок пока нет
- Answer To CommentsДокумент6 страницAnswer To CommentsKumar DasОценок пока нет
- Evidence From Community Level Inputs To Improve The NewBorn HealthДокумент19 страницEvidence From Community Level Inputs To Improve The NewBorn HealthKumar DasОценок пока нет
- Late Course Change FormДокумент2 страницыLate Course Change FormKumar DasОценок пока нет
- A Randomized Breast Feeding ProgrammeДокумент5 страницA Randomized Breast Feeding ProgrammeKumar DasОценок пока нет
- Because We All Know That Vaccines Are An Extremely Effective Public Health Tool': Path Dependency, H1N1 and The World Health OrganisationДокумент18 страницBecause We All Know That Vaccines Are An Extremely Effective Public Health Tool': Path Dependency, H1N1 and The World Health OrganisationKumar DasОценок пока нет
- Bihar Nutrition Stakeholder AnalysisДокумент18 страницBihar Nutrition Stakeholder AnalysisKumar DasОценок пока нет
- Breast Feeding Peer CouncellingДокумент22 страницыBreast Feeding Peer CouncellingKumar DasОценок пока нет
- 10-31-2015 - A Multi-DiДокумент18 страниц10-31-2015 - A Multi-DiKumar DasОценок пока нет
- CBM - Policy BriefДокумент3 страницыCBM - Policy BriefKumar DasОценок пока нет
- Transforming Agriculture Extension - Public Sector Reforms in Agriculture Extension in IndiaДокумент8 страницTransforming Agriculture Extension - Public Sector Reforms in Agriculture Extension in IndiaKumar DasОценок пока нет
- Sexuality, Poverty and Food SecurityДокумент8 страницSexuality, Poverty and Food SecurityKumar DasОценок пока нет
- Effect of community-based newborn interventions in BangladeshДокумент9 страницEffect of community-based newborn interventions in BangladeshKumar DasОценок пока нет
- Concept Note For HNS Integration ModelДокумент6 страницConcept Note For HNS Integration ModelKumar DasОценок пока нет
- Routine Immunization 28.05.2014 PDFДокумент5 страницRoutine Immunization 28.05.2014 PDFKumar DasОценок пока нет
- Integration of Health Nutrition and Sanitation Agenda in JEEViKA 01.08.2014Документ14 страницIntegration of Health Nutrition and Sanitation Agenda in JEEViKA 01.08.2014Kumar DasОценок пока нет
- Empowerment Through Market Led DevelopmentДокумент9 страницEmpowerment Through Market Led DevelopmentKumar DasОценок пока нет
- Sexuality - A Critical Link To Poverty and Food SecurityДокумент14 страницSexuality - A Critical Link To Poverty and Food SecurityKumar DasОценок пока нет
- Sexuality, Poverty and Food SecurityДокумент8 страницSexuality, Poverty and Food SecurityKumar DasОценок пока нет
- ReportДокумент24 страницыReportKumar DasОценок пока нет
- Monitoring and Evaluation ImpactДокумент22 страницыMonitoring and Evaluation ImpactKumar Das100% (1)
- Sexuality - A Critical Link To Poverty and Food SecurityДокумент14 страницSexuality - A Critical Link To Poverty and Food SecurityKumar DasОценок пока нет
- Chinese AidДокумент8 страницChinese AidKumar DasОценок пока нет
- The Factors Impacting Adoption of Agricultural Technology - The Case of Uttar Pradesh IndiaДокумент9 страницThe Factors Impacting Adoption of Agricultural Technology - The Case of Uttar Pradesh IndiaKumar DasОценок пока нет
- Ritin Kumar Srivastava Block No. 31/4, Kabeer Nagar Colony: TH THДокумент3 страницыRitin Kumar Srivastava Block No. 31/4, Kabeer Nagar Colony: TH THswapnilkhadke89Оценок пока нет
- The Dog Encyclopedia (VetBooks - Ir)Документ362 страницыThe Dog Encyclopedia (VetBooks - Ir)miki122295% (22)
- Fire Prevention and Response Plan for Greenergie PlantДокумент8 страницFire Prevention and Response Plan for Greenergie PlantMelba MangabatОценок пока нет
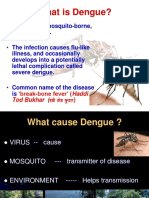
- Dengue PreventionДокумент30 страницDengue PreventionJaneshaОценок пока нет
- Career GoalДокумент9 страницCareer GoalaphonorsstudytimeОценок пока нет
- Understanding The Self: Sexual SelfДокумент13 страницUnderstanding The Self: Sexual SelfJustin UyОценок пока нет
- Gram Negative CocciДокумент14 страницGram Negative CocciRachel Marie M. GaniaОценок пока нет
- Stress ManagementДокумент54 страницыStress ManagementjomelofillartosОценок пока нет
- Surfactantreplacementtherapy 160926164838Документ33 страницыSurfactantreplacementtherapy 160926164838revathidadam55555Оценок пока нет
- Urine As Pesticide and FertilizerДокумент16 страницUrine As Pesticide and FertilizerMark Ronald Samijon Manseguiao100% (1)
- Presentation Datin PH WongДокумент38 страницPresentation Datin PH WongFakhriyahNur IbrahimОценок пока нет
- How Much Does A Kidney Transplant Cost?Документ1 страницаHow Much Does A Kidney Transplant Cost?Ivan RodriguezОценок пока нет
- Egg Preparation: Egg - in Cookery, Egg Refers To Poultry orДокумент3 страницыEgg Preparation: Egg - in Cookery, Egg Refers To Poultry orRenz GregorioОценок пока нет
- Improve Your Deadlift 12-Week TRAINERДокумент23 страницыImprove Your Deadlift 12-Week TRAINERNagan Ecomagu100% (1)
- Sip ProposalДокумент6 страницSip ProposalStephanie CulalaОценок пока нет
- Hydrochloric Acid 30-35%Документ17 страницHydrochloric Acid 30-35%Wong Peng ChiongОценок пока нет
- Ab Dental Catalogo 2017Документ82 страницыAb Dental Catalogo 2017ilich sevillaОценок пока нет
- RD Information: Eligibility Requirements For RD ExamДокумент30 страницRD Information: Eligibility Requirements For RD ExamAjay KumarОценок пока нет
- Gynaecological Clinical Guidelines - NHSДокумент39 страницGynaecological Clinical Guidelines - NHSvchendilОценок пока нет
- Color PsychologyДокумент10 страницColor PsychologyRemya100% (1)
- Gima CatalogДокумент84 страницыGima Catalogsara şovreОценок пока нет
- Plagiarism - Paraphrase and Summary HandoutДокумент10 страницPlagiarism - Paraphrase and Summary HandoutTika VirginiyaОценок пока нет
- Gabriel's Rage: The Horrors of Ward 13Документ59 страницGabriel's Rage: The Horrors of Ward 13Branislav IvanovicОценок пока нет
- Ivf Center PDFДокумент15 страницIvf Center PDFKinjalОценок пока нет
- In Search of Respect CH 9Документ11 страницIn Search of Respect CH 9Jared Micahl McDuffeyОценок пока нет
- HLTH 308 Group Assignment 1Документ9 страницHLTH 308 Group Assignment 1api-681327493Оценок пока нет
- Manalo-John, EssayДокумент11 страницManalo-John, EssayJohn ManaloОценок пока нет
- Complementary and Alternative TherapiesДокумент67 страницComplementary and Alternative TherapiesRachel PerisadeОценок пока нет