Вам также может понравиться
- MAIB - Collision Due To Anchor DragДокумент16 страницMAIB - Collision Due To Anchor DragBinh Pham100% (1)
- Understanding Mooring IncideДокумент8 страницUnderstanding Mooring IncideIan MaldonadoОценок пока нет
- Add MassДокумент9 страницAdd MassjamesОценок пока нет
- MAIB Report On MSC Napoli CasualtyДокумент56 страницMAIB Report On MSC Napoli CasualtyBinh PhamОценок пока нет
- Staad Pro TutorialsДокумент17 страницStaad Pro Tutorialsrandhir981Оценок пока нет
- Failure CPP - Key BoraДокумент12 страницFailure CPP - Key BoraBinh PhamОценок пока нет
- UnderstandingMooringIncidents PDFДокумент8 страницUnderstandingMooringIncidents PDFBinh PhamОценок пока нет
- Hoegh Osaka MAIB ReportДокумент86 страницHoegh Osaka MAIB ReportIWCPOnlineОценок пока нет
- Technical Investigation Accident Twin Crane LiftДокумент6 страницTechnical Investigation Accident Twin Crane LiftBinh PhamОценок пока нет
- STRIKING of OSV Maersk DetectorДокумент45 страницSTRIKING of OSV Maersk DetectorBinh PhamОценок пока нет
- Technical Reference 2007 CompleteДокумент782 страницыTechnical Reference 2007 CompleteIvan GradОценок пока нет
- UKOOA FPSO Design Guidance NotesДокумент176 страницUKOOA FPSO Design Guidance Notesnazwan14100% (5)
- Dutch NavigatorДокумент66 страницDutch NavigatorBinh Pham100% (1)
- Chief Ton TugДокумент69 страницChief Ton TugBinh PhamОценок пока нет
- API Deepwater Standards PosterДокумент1 страницаAPI Deepwater Standards PosterBoonme ChinnaboonОценок пока нет
- Sten A Voyager ReportДокумент45 страницSten A Voyager ReportBinh PhamОценок пока нет
- Collission RickmersDubaiДокумент88 страницCollission RickmersDubaiBinh Pham100% (1)
- Wave Drift Forces and Responses in Deep Water and Extreme Environmental ConditionsДокумент4 страницыWave Drift Forces and Responses in Deep Water and Extreme Environmental Conditionssaeed-21Оценок пока нет
- Tie-In Spool - A Verification Study (MSC)Документ213 страницTie-In Spool - A Verification Study (MSC)Binh PhamОценок пока нет
- Annabella ReportДокумент40 страницAnnabella ReportBinh PhamОценок пока нет
- Failure CPP - Key BoraДокумент12 страницFailure CPP - Key BoraBinh PhamОценок пока нет
- DP class notation guide for major classification societiesДокумент1 страницаDP class notation guide for major classification societiesswapneel_kulkarniОценок пока нет
- Otc19607 About API RP 2skДокумент12 страницOtc19607 About API RP 2skBinh PhamОценок пока нет
- Dynamic Positioning SimulatorДокумент79 страницDynamic Positioning Simulatortm5u2r100% (3)
- Skandi HerculesДокумент9 страницSkandi Herculesiw2fualОценок пока нет
- Drillship Hull Structure Design and AnalysisДокумент214 страницDrillship Hull Structure Design and AnalysisBinh PhamОценок пока нет
- Classification of Mooring SystemsДокумент38 страницClassification of Mooring SystemsBinh Pham100% (1)
- Petroleum Engineering Station Keeping GuideДокумент41 страницаPetroleum Engineering Station Keeping GuideBinh PhamОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Advisory Circular AC 139.C-07 v1.0: Strength Rating of Aerodrome PavementsДокумент37 страницAdvisory Circular AC 139.C-07 v1.0: Strength Rating of Aerodrome PavementsWilder Francisco Grández VenturaОценок пока нет
- Cubigel Catalogo - 27 - 05 - 10 - IIДокумент68 страницCubigel Catalogo - 27 - 05 - 10 - IItempo345100% (1)
- Arif Corporation SDN BHDДокумент2 страницыArif Corporation SDN BHDMOHD NAIM MOKSIN HUSSINОценок пока нет
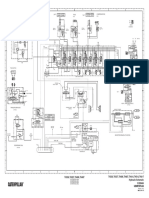
- TH336, TH337, TH406, TH407, TH414, TH514, TH417 Hydraulic Schematic TH336, TH337, TH406, TH407Документ2 страницыTH336, TH337, TH406, TH407, TH414, TH514, TH417 Hydraulic Schematic TH336, TH337, TH406, TH407مهدي شقرونОценок пока нет
- G450 Cockpit Lay OutДокумент1 страницаG450 Cockpit Lay OutFaisal Majeed100% (1)
- All About Air AsiaДокумент68 страницAll About Air AsiaAkmar Majuri50% (2)
- A2 Shipboard Fittings and Supporting Hull Structures Associated With Towing and Mooring On Conventional Vessels A2Документ6 страницA2 Shipboard Fittings and Supporting Hull Structures Associated With Towing and Mooring On Conventional Vessels A2tonyОценок пока нет
- BOP Category GuideДокумент29 страницBOP Category GuidePaul JohnОценок пока нет
- Taramps TS800X4Документ8 страницTaramps TS800X4VOLKSOUND Ailton Jr.Оценок пока нет
- 1994 Prowler NewДокумент66 страниц1994 Prowler Newrs657100% (5)
- 4509022956Документ4 страницы4509022956pratiwioktoritaymailОценок пока нет
- PASSAT 3B AdaptionsДокумент4 страницыPASSAT 3B AdaptionsCristian SindieОценок пока нет
- Automotive Design Course IndiaДокумент17 страницAutomotive Design Course Indiamq23Оценок пока нет
- India A Develop Nation by 2047Документ29 страницIndia A Develop Nation by 2047sudhirОценок пока нет
- EuropeДокумент100 страницEuropeRamesh PerumalОценок пока нет
- Site Report Anguilla Shipwreck SurveyДокумент59 страницSite Report Anguilla Shipwreck SurveylilliazevedoОценок пока нет
- In-Situ Burning of Oil in Ships or Other Vessels: Standard Guide ForДокумент6 страницIn-Situ Burning of Oil in Ships or Other Vessels: Standard Guide ForAhmad Zubair RasulyОценок пока нет
- Universal Joint 2014 GMBДокумент49 страницUniversal Joint 2014 GMB'RomОценок пока нет
- Husqvarna 2003 SM WRE 125 ManualДокумент2 страницыHusqvarna 2003 SM WRE 125 ManualNdae IskandarОценок пока нет
- Automated storage and retrieval systems (AS/RS) for efficient warehouse managementДокумент26 страницAutomated storage and retrieval systems (AS/RS) for efficient warehouse managementEusebiu PetuОценок пока нет
- Radio and Player Wiring DiagramДокумент4 страницыRadio and Player Wiring DiagramHerson EscobarОценок пока нет
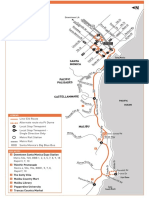
- Route 534 Santa Monica MalibuДокумент3 страницыRoute 534 Santa Monica MalibudazulzulОценок пока нет
- Sept06 NoblejackupДокумент3 страницыSept06 NoblejackupmanhngoducОценок пока нет
- Barilla Case Study SolutionДокумент6 страницBarilla Case Study SolutionJayati AgrawalОценок пока нет
- Laying of Underground CablesДокумент17 страницLaying of Underground CablesMohammed K. HayderОценок пока нет
- December Ka TicketДокумент1 страницаDecember Ka TicketShirsh SawarnaОценок пока нет
- Evo7 GtaДокумент9 страницEvo7 GtaBhirawich PholpokeОценок пока нет
- BW MapДокумент2 страницыBW MapDamon MeddingsОценок пока нет
- 2 Sample SHS G11 Research Paper by Turingan, JohnДокумент42 страницы2 Sample SHS G11 Research Paper by Turingan, JohnJedí BelanoОценок пока нет
- FKSM 71-8 June 2007 Heavy and Infantry Brigade Combat TeamДокумент124 страницыFKSM 71-8 June 2007 Heavy and Infantry Brigade Combat TeamPaul D Carrier100% (3)