Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Stockard Tests UE & LE TДокумент4 страницыStockard Tests UE & LE TLinh HoangОценок пока нет
- Virtual Pig Dissection Worksheet 06-07 2Документ6 страницVirtual Pig Dissection Worksheet 06-07 2api-255054890Оценок пока нет
- St. Victoria Hospital Nursing Service Ward DeptДокумент50 страницSt. Victoria Hospital Nursing Service Ward DeptPat MagpaliОценок пока нет
- Lovenox (Enoxaparin)Документ1 страницаLovenox (Enoxaparin)E100% (1)
- (2017) OGUNYEMI, Boluwaji MILLER-MONTHROPE, Yvette. The State of Ethnic Dermatology in CanadaДокумент3 страницы(2017) OGUNYEMI, Boluwaji MILLER-MONTHROPE, Yvette. The State of Ethnic Dermatology in CanadaCassandra VérasОценок пока нет
- Mercy Obstetric Triage OTDA A Standardised Approach To Care CHA SlidesДокумент28 страницMercy Obstetric Triage OTDA A Standardised Approach To Care CHA Slidessaepulloh bin amingОценок пока нет
- Practical Medical Oncology Textbook (Antonio Russo, Marc Peeters, Lorena Incorvaia Etc.)Документ1 104 страницыPractical Medical Oncology Textbook (Antonio Russo, Marc Peeters, Lorena Incorvaia Etc.)Paolo FassinaОценок пока нет
- Data Thermal Printer CSДокумент24 страницыData Thermal Printer CSDedy Chandra HariyonoОценок пока нет
- KlikBCA Individual Save PageДокумент1 страницаKlikBCA Individual Save PageDedy Chandra HariyonoОценок пока нет
- ManagementДокумент1 страницаManagementDedy Chandra HariyonoОценок пока нет
- Promoting Products: Brand of Product Product Category Company ShapeДокумент2 страницыPromoting Products: Brand of Product Product Category Company ShapeDedy Chandra HariyonoОценок пока нет
- Manufacturing and ServicesДокумент1 страницаManufacturing and ServicesDedy Chandra HariyonoОценок пока нет
- CV (Yessy)Документ1 страницаCV (Yessy)Dedy Chandra HariyonoОценок пока нет
- CV (Yessy)Документ1 страницаCV (Yessy)Dedy Chandra HariyonoОценок пока нет
- Manufacturing and ServicesДокумент1 страницаManufacturing and ServicesDedy Chandra HariyonoОценок пока нет
- Manufacturing and ServicesДокумент1 страницаManufacturing and ServicesDedy Chandra HariyonoОценок пока нет
- Promoting Products: Brand of Product Product Category Company ShapeДокумент2 страницыPromoting Products: Brand of Product Product Category Company ShapeDedy Chandra HariyonoОценок пока нет
- KlikBCA Individual Save Page - JPGGДокумент1 страницаKlikBCA Individual Save Page - JPGGDedy Chandra HariyonoОценок пока нет
- CV (Yessy)Документ1 страницаCV (Yessy)Dedy Chandra HariyonoОценок пока нет
- Pericarditis and Pericardial EffusionДокумент31 страницаPericarditis and Pericardial EffusionDedy Chandra HariyonoОценок пока нет
- CardiomyopathyДокумент23 страницыCardiomyopathyDedy Chandra HariyonoОценок пока нет
- 1015Документ7 страниц1015Bang DeОценок пока нет
- TorrentДокумент1 страницаTorrentDedy Chandra HariyonoОценок пока нет
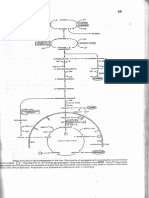
- Glukoneogenesis (Dr. Hairrudin)Документ1 страницаGlukoneogenesis (Dr. Hairrudin)devezzfilОценок пока нет
- TorrentДокумент1 страницаTorrentDedy Chandra HariyonoОценок пока нет
- Makanan PengawetДокумент6 страницMakanan PengawetDedy Chandra HariyonoОценок пока нет
- Herbalife 1 - Slimming at All Costs: HerbalifeÒ-induced Liver InjuryДокумент3 страницыHerbalife 1 - Slimming at All Costs: HerbalifeÒ-induced Liver InjuryMohammed AyubОценок пока нет
- Insya AllahДокумент1 страницаInsya AllahDedy Chandra HariyonoОценок пока нет
- (José Almeida) Atlas of Endovascular Venous SurgeДокумент516 страниц(José Almeida) Atlas of Endovascular Venous SurgeTa TaОценок пока нет
- Placenta Previa (New) - 1Документ32 страницыPlacenta Previa (New) - 1Ibrahim ZainabОценок пока нет
- Ethicon Suture & Needles wall chart (2 pages)Документ2 страницыEthicon Suture & Needles wall chart (2 pages)andy liОценок пока нет
- Guide to Head and Neck DiseasesДокумент47 страницGuide to Head and Neck DiseasesDonna LabaniegoОценок пока нет
- A Practical Guide to HPIДокумент11 страницA Practical Guide to HPIMichael NyaongoОценок пока нет
- Eyelid Trauma and Orbital FracturesДокумент16 страницEyelid Trauma and Orbital FracturesFachroni Agim RahmanОценок пока нет
- Officinalis) : Lavender (LavandulaДокумент3 страницыOfficinalis) : Lavender (LavandulaMacsim RoxanaОценок пока нет
- Lower Extremity Venous Duplex USДокумент6 страницLower Extremity Venous Duplex USjmg_mdОценок пока нет
- Labor and Birth Process 3 Stage & 4 Stage: RD THДокумент23 страницыLabor and Birth Process 3 Stage & 4 Stage: RD THبشائر حمادةОценок пока нет
- Anesthesia Professional Coding For McKesson Anesthesia Care™Документ2 страницыAnesthesia Professional Coding For McKesson Anesthesia Care™McKesson Surgical SolutionsОценок пока нет
- Report On The Hospital VisitДокумент4 страницыReport On The Hospital VisitSolanki PrakashОценок пока нет
- Lath AДокумент118 страницLath AManish PandeyОценок пока нет
- Tugas Dr. Domingos Da SilvaДокумент6 страницTugas Dr. Domingos Da Silvadenilay richardoОценок пока нет
- A Study On "Contract Labour"Документ67 страницA Study On "Contract Labour"Phani BabuОценок пока нет
- Population Welfare Program and ServicesДокумент57 страницPopulation Welfare Program and Servicesadeel_khan_48Оценок пока нет
- Eswl 1Документ33 страницыEswl 1G Vignesh GvsОценок пока нет
- Nelson MCQ PDFДокумент595 страницNelson MCQ PDFPavan Kumar100% (5)
- Artificial Limb Research in BangladeshДокумент5 страницArtificial Limb Research in BangladeshMd IslamОценок пока нет
- Nursing Bullets Fundamentals GuideДокумент89 страницNursing Bullets Fundamentals GuideJek NevadoОценок пока нет
- ICRA Form v08.07Документ5 страницICRA Form v08.07Indra Juang Putra HarefaОценок пока нет
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveДокумент5 страницCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaОценок пока нет
- Biodata: PARGANAS, KOLKATA-700102, West BengalДокумент3 страницыBiodata: PARGANAS, KOLKATA-700102, West BengalTina lovelyОценок пока нет
- Treatment and Management AppendicitisДокумент3 страницыTreatment and Management Appendicitisruthjoy23upgirlОценок пока нет