Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Five Tibetan RitesДокумент14 страницThe Five Tibetan Ritesreha-kaubaОценок пока нет
- Retire HappyДокумент266 страницRetire HappyEdsel Llave100% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hypothesis Testing Complete SlidesДокумент54 страницыHypothesis Testing Complete Slidesghabel11Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Non-Communicable Diseases and Health Systems Reform in Low and Middle-Income Countries (WP13)Документ24 страницыNon-Communicable Diseases and Health Systems Reform in Low and Middle-Income Countries (WP13)Nossal Institute for Global HealthОценок пока нет
- BCPS Study 10monthДокумент5 страницBCPS Study 10monthMagdy Ali ELsherbenyОценок пока нет
- Half Marathon TrainingДокумент27 страницHalf Marathon TrainingCarlos Pizano Martínez100% (1)
- Sugar Content of FruitДокумент6 страницSugar Content of Fruitjose lourencoОценок пока нет
- NUTRI Quiz BeeДокумент5 страницNUTRI Quiz Beejheng san diegoОценок пока нет
- Physical Fitness Test Score CardДокумент1 страницаPhysical Fitness Test Score Cardmarjun catan100% (1)
- Tacfit 4 DietДокумент13 страницTacfit 4 Dietsaz08100% (2)
- DRUG STUDY EpinephrineДокумент2 страницыDRUG STUDY EpinephrineCarlo Francisco D. Canto78% (9)
- Shape Malaysia July 2014Документ100 страницShape Malaysia July 2014ZirahNamiaОценок пока нет
- Resistant Starch As Functional IngredientДокумент47 страницResistant Starch As Functional IngredientGhulam Mustafa0% (2)
- Men's Health 01.02 2019Документ118 страницMen's Health 01.02 2019Mike MarineОценок пока нет
- Ccebdm Module 8Документ140 страницCcebdm Module 8AnkurОценок пока нет
- CaptoprilДокумент13 страницCaptoprilMagdy Ali ELsherbenyОценок пока нет
- Propylthiouracil 2Документ14 страницPropylthiouracil 2Magdy Ali ELsherbenyОценок пока нет
- PROPYLTHIOURACILДокумент35 страницPROPYLTHIOURACILMagdy Ali ELsherbenyОценок пока нет
- Mayoclinproc 86 2 013 PDFДокумент12 страницMayoclinproc 86 2 013 PDFMagdy Ali ELsherbenyОценок пока нет
- Wiki Human HomeostasisДокумент5 страницWiki Human HomeostasisMagdy Ali ELsherbenyОценок пока нет
- Fitness Progress Chart For Men (Metric) 1Документ4 страницыFitness Progress Chart For Men (Metric) 1John Gaming444Оценок пока нет
- Modul Anatomy Blok 2-2Документ46 страницModul Anatomy Blok 2-2AyuОценок пока нет
- Ch12 Basic Syrups Creams and SaucesДокумент18 страницCh12 Basic Syrups Creams and Saucessurapong2005Оценок пока нет
- ICT Project: "Deterrent Malnutrition Among Filipino Children"Документ7 страницICT Project: "Deterrent Malnutrition Among Filipino Children"Janea ArinyaОценок пока нет
- Sleeve-Gastrectomy 2011 BrethauerДокумент15 страницSleeve-Gastrectomy 2011 BrethauerDavid Schnettler RodriguezОценок пока нет
- Super Size MeДокумент2 страницыSuper Size MeJosep VlcОценок пока нет
- Circulatory System KNP NotesДокумент3 страницыCirculatory System KNP Notesmelindamd8Оценок пока нет
- Hormon Reproduksi: Dr. Septi Handayani, M.SiДокумент133 страницыHormon Reproduksi: Dr. Septi Handayani, M.SipiniОценок пока нет
- Preoperative Assessment in Diabetic PatientsДокумент2 страницыPreoperative Assessment in Diabetic PatientsShilpa Pradhan100% (1)
- Mapeh 10-1st Quarter NewДокумент3 страницыMapeh 10-1st Quarter NewJinkie Joyce CuagdanОценок пока нет
- Ehy 339Документ98 страницEhy 339Xarisis IoannisОценок пока нет
- CLA N Lipid in RuminantsДокумент46 страницCLA N Lipid in RuminantsTamii MatulОценок пока нет
- Latihan Soal UN Bahasa Inggris SMP 2017Документ11 страницLatihan Soal UN Bahasa Inggris SMP 2017jenifer tiffany100% (1)
- Paula Mcclusky Aprn PresentationДокумент18 страницPaula Mcclusky Aprn Presentationapi-676449505Оценок пока нет
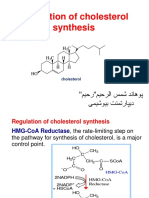
- Regulation of Cholesterol SynthesisДокумент20 страницRegulation of Cholesterol SynthesisHusnaОценок пока нет
- THE STARCH SOLUTION: The Low Fat Whole Foods Plant Based DietДокумент2 страницыTHE STARCH SOLUTION: The Low Fat Whole Foods Plant Based DietSalman khanОценок пока нет