Вам также может понравиться
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Firefighter 1 Academy Information - Spring 2018Документ9 страницFirefighter 1 Academy Information - Spring 2018venggyОценок пока нет
- Prehospital Trauma Life Support (PHTLS) Training of Ambulance Caregivers and Impact On Survival of Trauma VictimsДокумент7 страницPrehospital Trauma Life Support (PHTLS) Training of Ambulance Caregivers and Impact On Survival of Trauma VictimsvenggyОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
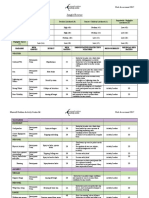
- Jungle Rescue: Marwell Outdoor Activity Centre Ltd. Risk Assessment 2017Документ7 страницJungle Rescue: Marwell Outdoor Activity Centre Ltd. Risk Assessment 2017venggyОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Recognizing and Responding To Aquatic Emergencies: - Swimming and Water SafetyДокумент28 страницRecognizing and Responding To Aquatic Emergencies: - Swimming and Water SafetyvenggyОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- 2 Climbing Equipment Safety4201Документ11 страниц2 Climbing Equipment Safety4201venggyОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- 119 434 1 PB PDFДокумент19 страниц119 434 1 PB PDFAnonymous nEQNlgbYQCОценок пока нет
- FileДокумент11 страницFilevenggyОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Balinese Culture: Dance, Drama, TextilesДокумент6 страницBalinese Culture: Dance, Drama, TextilesvenggyОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Implement Entrepreneurship Daily with MLM BusinessДокумент2 страницыImplement Entrepreneurship Daily with MLM BusinessvenggyОценок пока нет
- 3D Topography Using Xara 3D & PhotoshopДокумент27 страниц3D Topography Using Xara 3D & PhotoshopvenggyОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- Diarrhea: Group 4: Surya Patricya Serikat Niscaya Theresia Yuni Venggy Reylandhie Yustina NayДокумент15 страницDiarrhea: Group 4: Surya Patricya Serikat Niscaya Theresia Yuni Venggy Reylandhie Yustina NayvenggyОценок пока нет
- Background: Pediatric Chickenpox Next Section: PathophysiologyДокумент12 страницBackground: Pediatric Chickenpox Next Section: PathophysiologyRachel Johann Aquinto100% (1)
- Threshold Reiki Reiki Ryoho HikkeiДокумент27 страницThreshold Reiki Reiki Ryoho HikkeiHarrison KoehliОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- AVSD - Revised VersionДокумент3 страницыAVSD - Revised Versiondr_IstiqlalMiftahulJannahОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- A Review of The Use of The Health Belief Model For Weight ManagementДокумент1 страницаA Review of The Use of The Health Belief Model For Weight ManagementpatresyaОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Tourettes SyndromeДокумент12 страницTourettes Syndromeapi-238788335Оценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- AHA ACLS Provider Manual $45Документ2 страницыAHA ACLS Provider Manual $45Jigar GandhiОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Rehab-U FreeMobilityEbook PDFДокумент10 страницRehab-U FreeMobilityEbook PDFTuteraipuni POTHIERОценок пока нет
- Surgical Approaches To The Skull BaseДокумент2 страницыSurgical Approaches To The Skull Baseİbrahim ErkutluОценок пока нет
- EmpiricalBasis GottmanДокумент10 страницEmpiricalBasis GottmanMundoSinViolenciaОценок пока нет
- MNA EnglishДокумент1 страницаMNA Englishdidik hariyadiОценок пока нет
- Nurs 205 Concept MapДокумент1 страницаNurs 205 Concept MapJami SpearsОценок пока нет
- Hospital Waste Water TreatmentДокумент5 страницHospital Waste Water TreatmentNP100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Aesthetic Jurnal PDFДокумент20 страницAesthetic Jurnal PDFTarrayuanaОценок пока нет
- Coding Handbook - Doc 6-16-09 Revised 8 14 09 AddДокумент52 страницыCoding Handbook - Doc 6-16-09 Revised 8 14 09 AddcindybevОценок пока нет
- Stabilisation and Safe Transport of The Critically Ill ChildДокумент9 страницStabilisation and Safe Transport of The Critically Ill ChildAdrian CraciunОценок пока нет
- Myopia ManualДокумент337 страницMyopia ManualRealPurgatory100% (1)
- MEDUMAT Standard 2 83700-ENДокумент16 страницMEDUMAT Standard 2 83700-ENJagath PrasangaОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Nada Lincomycyn and Espectynomycin Solubleucm061812Документ4 страницыNada Lincomycyn and Espectynomycin Solubleucm061812laurz95Оценок пока нет
- FIRST EVER Cold Therapy Certification Seminar in Vienna! REGISTER NOW!Документ5 страницFIRST EVER Cold Therapy Certification Seminar in Vienna! REGISTER NOW!zadanliran100% (1)
- Hyspin AWH-M 32Документ4 страницыHyspin AWH-M 32bboy640Оценок пока нет
- Anc 0001 0009 0151Документ42 страницыAnc 0001 0009 0151ManhaОценок пока нет
- The Egyptian Heart Journal: Haitham Galal Mohammed, Adel Mohamed ShabanaДокумент6 страницThe Egyptian Heart Journal: Haitham Galal Mohammed, Adel Mohamed ShabanaDaniel Zagoto100% (1)
- Fast Food Industry ResearchДокумент13 страницFast Food Industry ResearchNaa Okaikor OkineОценок пока нет
- Research ArticleДокумент4 страницыResearch ArticleBharathi RagavanОценок пока нет
- Rexulti PIДокумент39 страницRexulti PIbenaw187Оценок пока нет
- Repertory: Information On Health Concerns in A Health DirectoryДокумент17 страницRepertory: Information On Health Concerns in A Health DirectoryShalinta Dubey SharmaОценок пока нет
- Practice Guidelines For The Diagnosis and Management of Aspergilosis 2016 Update by AmericaДокумент60 страницPractice Guidelines For The Diagnosis and Management of Aspergilosis 2016 Update by AmericaNur Prasetyo Nugroho100% (1)
- Gastrointestinal System Ppt.-NewДокумент117 страницGastrointestinal System Ppt.-NewFatima Syed100% (3)
- MedicalДокумент3 страницыMedicalmumtazkauser74Оценок пока нет
- Harvard Catalyst - Medical Marijuana A Status Report - Jeffrey Miron - Gladys Varela 12-6-11Документ29 страницHarvard Catalyst - Medical Marijuana A Status Report - Jeffrey Miron - Gladys Varela 12-6-11valuzzzzОценок пока нет