Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Anaemia in PregnancyДокумент28 страницAnaemia in PregnancyUsman G. HingoroОценок пока нет
- Management of Cardiac Arrest in The Pregnant PatientДокумент11 страницManagement of Cardiac Arrest in The Pregnant PatientHeath HensleyОценок пока нет
- Bureau Circular 5 S 1997Документ39 страницBureau Circular 5 S 1997mrk_rlndОценок пока нет
- Globalization and BreastfeedingДокумент52 страницыGlobalization and BreastfeedingMichele RochaОценок пока нет
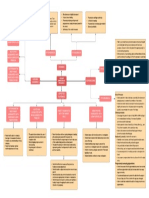
- A2 Concept MapДокумент1 страницаA2 Concept MapMyfanway Am-isОценок пока нет
- Proc Edur e 5 4 3 2 1: Prenatal Check-UpДокумент60 страницProc Edur e 5 4 3 2 1: Prenatal Check-UpCharlie DyОценок пока нет
- History Examination of Gynecology and Obstetrics PatientsДокумент3 страницыHistory Examination of Gynecology and Obstetrics PatientsAgus WijayaОценок пока нет
- Paediatric Assessment FormДокумент4 страницыPaediatric Assessment Formdrrajmptn90% (30)
- Oecd/Ocde 414: Oecd Guideline For Testing of ChemicalsДокумент14 страницOecd/Ocde 414: Oecd Guideline For Testing of ChemicalsDiana IrimescuОценок пока нет
- QuestionДокумент6 страницQuestiontravelbeeОценок пока нет
- Research Final Proposal Printed Original Yegna Ye Group TwoДокумент62 страницыResearch Final Proposal Printed Original Yegna Ye Group TwoMulugeta AbenehОценок пока нет
- GupisoneДокумент7 страницGupisoneahibba.03862Оценок пока нет
- Viral Hepatitis in Pregnancy: DR Eleni Nastouli Consultant in Virology and Paediatric Infectious DiseasesДокумент34 страницыViral Hepatitis in Pregnancy: DR Eleni Nastouli Consultant in Virology and Paediatric Infectious Diseasesrilla saeliputriОценок пока нет
- Does Suture Material Affect Uterine Scar Healing After Cesarean Section? Results From A Randomized Controlled TrialДокумент9 страницDoes Suture Material Affect Uterine Scar Healing After Cesarean Section? Results From A Randomized Controlled TrialMariana HernandezОценок пока нет
- Kareena Kapoor Khan S Pregnancy Bible The Ultimate Manual For MomsДокумент314 страницKareena Kapoor Khan S Pregnancy Bible The Ultimate Manual For Momsk k82% (11)
- College of Our Lady of Mt. Carmel: Midwifery DepartmentДокумент10 страницCollege of Our Lady of Mt. Carmel: Midwifery DepartmentMA. JYRELL BONITOОценок пока нет
- Term Paper Early PregnancyДокумент7 страницTerm Paper Early Pregnancyaehupavkg100% (1)
- HMOLEДокумент34 страницыHMOLEZuellen Mae Garapan BedañoОценок пока нет
- MSC Nursing RS3&RS4Документ21 страницаMSC Nursing RS3&RS4Atif PashaОценок пока нет
- 2011 Coast Spa Owner's ManualДокумент20 страниц2011 Coast Spa Owner's ManualTom KakanowskiОценок пока нет
- Maternity and Paternity LeaveДокумент4 страницыMaternity and Paternity LeavePerry YapОценок пока нет
- Clinical Nutrition: Aisha Mansoor Ali, Abdulaziz Alobaid, Tasnim Nidal Malhis, Ahmad Fawzi KhattabДокумент7 страницClinical Nutrition: Aisha Mansoor Ali, Abdulaziz Alobaid, Tasnim Nidal Malhis, Ahmad Fawzi KhattabDewi Retno AstutyОценок пока нет
- Maternal and Child Healthe Nursing MCQ 6Документ18 страницMaternal and Child Healthe Nursing MCQ 6shanika100% (1)
- ACOG-49 Dystocia and Augmentation of LaborДокумент10 страницACOG-49 Dystocia and Augmentation of LaborAngeredYetiОценок пока нет
- Direct and Indirect SpeechДокумент3 страницыDirect and Indirect SpeechLenni apriani TafonaoОценок пока нет
- The Ila-Speaking Peoples of Northern RhodesiaДокумент333 страницыThe Ila-Speaking Peoples of Northern RhodesiadanckckОценок пока нет
- Recommendations For Well-Woman Care - A Well-Woman Chart Clinical Summary TablesДокумент41 страницаRecommendations For Well-Woman Care - A Well-Woman Chart Clinical Summary TablesRïta Câro SantösОценок пока нет
- Premature Baby EssayДокумент12 страницPremature Baby Essayapi-509682910Оценок пока нет
- Pediatric Lyme DiseaseДокумент52 страницыPediatric Lyme DiseaseWanda BakerОценок пока нет
- Medical Termination of Pregnancy (MTP) Amendment Act, 2021: Why in NewsДокумент4 страницыMedical Termination of Pregnancy (MTP) Amendment Act, 2021: Why in NewsVivek GiriОценок пока нет