Вам также может понравиться
- Antpyretic-Analgesic and Antinlammatory DrugsДокумент38 страницAntpyretic-Analgesic and Antinlammatory DrugskasondaОценок пока нет
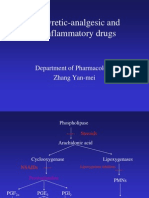
- Antipyretic-Analgesic and Antiinflammatory Drugs: Department of Pharmacology Zhang Yan-MeiДокумент39 страницAntipyretic-Analgesic and Antiinflammatory Drugs: Department of Pharmacology Zhang Yan-MeiIshu SethiОценок пока нет
- Anti Inflamatory Drugs AINSДокумент39 страницAnti Inflamatory Drugs AINSEl FaroukОценок пока нет
- Antipyretic-Analgesic and Antiinflammatory DrugsДокумент46 страницAntipyretic-Analgesic and Antiinflammatory DrugsAYU SUKARNI PUTRIОценок пока нет
- NSAIDSДокумент38 страницNSAIDSShahmir KhanОценок пока нет
- Analgesics: Non-Steroidal Anti-Inflammatory Drugs andДокумент8 страницAnalgesics: Non-Steroidal Anti-Inflammatory Drugs andWilliam C ChishaОценок пока нет
- NSAID Mechanism and UsesДокумент11 страницNSAID Mechanism and UsesSuranjan GhoshОценок пока нет
- Anti Pyretic 2013Документ15 страницAnti Pyretic 2013Faizah Al GhamdiОценок пока нет
- NSAIDs: Mechanisms, Effects and UsesДокумент43 страницыNSAIDs: Mechanisms, Effects and UsesRitu ShewaniОценок пока нет
- Kharkov National Medical University Department of Pharmacology Lecture on Anti-inflammatory DrugsДокумент82 страницыKharkov National Medical University Department of Pharmacology Lecture on Anti-inflammatory DrugsHerry HendrayadiОценок пока нет
- 3 Analgesic Anitpyretic InfamДокумент10 страниц3 Analgesic Anitpyretic InfamAnonymous dRAu54Оценок пока нет
- Guide to NSAIDs (Non-Steroidal Anti-Inflammatory DrugsДокумент40 страницGuide to NSAIDs (Non-Steroidal Anti-Inflammatory DrugsHarini Bala100% (1)
- Cefradime, Paracetamol, KetorolacДокумент10 страницCefradime, Paracetamol, KetorolacMae_Sheryn_Lip_1795Оценок пока нет
- PAIN ControllersДокумент39 страницPAIN ControllersAyro Business CenterОценок пока нет
- Week 9 - Course Task - Case Analysis Renal DisordersДокумент4 страницыWeek 9 - Course Task - Case Analysis Renal DisordersJohnmarkLorenzanaRoveroОценок пока нет
- Anti-Inflammatory Drugs Class Notes 2023Документ82 страницыAnti-Inflammatory Drugs Class Notes 2023Jacob MasikaОценок пока нет
- Treatment of Acute GoutДокумент38 страницTreatment of Acute GoutAnoop PkОценок пока нет
- Bp1 Sgd1: TopicsДокумент7 страницBp1 Sgd1: TopicsAlan Joseph BaldovinoОценок пока нет
- NSAIDsДокумент12 страницNSAIDsjelly100% (1)
- Drug Study Effects and UsesДокумент11 страницDrug Study Effects and UsesVincent QuitorianoОценок пока нет
- Drug 25Документ17 страницDrug 25carol_gigliotti24100% (1)
- Penyakit Tersering Di PuskesmasДокумент5 страницPenyakit Tersering Di PuskesmasRama Al MaduriОценок пока нет
- pharamcology unit 10 answersДокумент13 страницpharamcology unit 10 answersLovren YoungОценок пока нет
- Relieve Angina & Congestive Heart FailureДокумент6 страницRelieve Angina & Congestive Heart FailureBij Hilario100% (1)
- Nursing Drug CardsДокумент32 страницыNursing Drug CardsJenna Rasmussen100% (3)
- NSAIDsДокумент34 страницыNSAIDsAliImadAlKhasaki75% (4)
- Anti Inflammatory DrugsДокумент82 страницыAnti Inflammatory DrugsShardendu MishraОценок пока нет
- Respiratory Tract PharmacologyДокумент68 страницRespiratory Tract PharmacologyRohaan SharmaОценок пока нет
- Prostaglandins and NSAIDs in InflammationДокумент21 страницаProstaglandins and NSAIDs in InflammationAmr SalemОценок пока нет
- NSADs: Non-Steroidal Anti-Inflammatory DrugsДокумент26 страницNSADs: Non-Steroidal Anti-Inflammatory DrugsSai Kishore K100% (1)
- B-Selective: I Group: Nonsteroidal Anti-Inflammatory Drugs (Nonsteroidal Ntiinflammatory)Документ6 страницB-Selective: I Group: Nonsteroidal Anti-Inflammatory Drugs (Nonsteroidal Ntiinflammatory)Moataz TrabehОценок пока нет
- Clinical Toxicology: Dep. of Biopharmaceutics and Clinical PharmacyДокумент32 страницыClinical Toxicology: Dep. of Biopharmaceutics and Clinical Pharmacymalak amerОценок пока нет
- Drug StudyДокумент19 страницDrug StudyCalimlim KimОценок пока нет
- NSAIDS 3, 4 SummaryДокумент29 страницNSAIDS 3, 4 SummaryAhmed ExaminationОценок пока нет
- Nsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyДокумент65 страницNsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyYousef JafarОценок пока нет
- GOUT PresentationДокумент24 страницыGOUT Presentationtasneemsofi100% (1)
- Analgesics: DR Mohammed Malik AfrozДокумент37 страницAnalgesics: DR Mohammed Malik AfrozMohee DawabshehОценок пока нет
- Lec9 د ذو الفقارДокумент4 страницыLec9 د ذو الفقارMohammed JaberОценок пока нет
- Drug StudyДокумент8 страницDrug StudyMike Faustino SolangonОценок пока нет
- Drug Study Gentamicin Sulfate and SalbutamolДокумент7 страницDrug Study Gentamicin Sulfate and SalbutamolEduardОценок пока нет
- Drug and NCPДокумент15 страницDrug and NCPgeelawlietОценок пока нет
- Drug Study CompilationДокумент9 страницDrug Study CompilationRene John FranciscoОценок пока нет
- NSAIDs: Non-steroidal Anti-inflammatory DrugsДокумент45 страницNSAIDs: Non-steroidal Anti-inflammatory DrugsArvi KhanОценок пока нет
- Nonsteroidal Antiinflammatory Drugs and Antipyretic - AnalgesicsДокумент28 страницNonsteroidal Antiinflammatory Drugs and Antipyretic - AnalgesicsJasveen SawhneyОценок пока нет
- Pharmacology of Adrenocorticoids and Adrenocorticotropic AntagonistsДокумент32 страницыPharmacology of Adrenocorticoids and Adrenocorticotropic AntagonistsJoyce VillanuevaОценок пока нет
- DrugsДокумент2 страницыDrugsgailannreyesОценок пока нет
- DrugsДокумент2 страницыDrugsgailannreyesОценок пока нет
- Kuliah Gouty ArthritisДокумент56 страницKuliah Gouty Arthritischrysandre100% (1)
- E Kart DrugsДокумент3 страницыE Kart DrugsNichole CastleОценок пока нет
- Drug StudyДокумент11 страницDrug StudyKaloy KamaoОценок пока нет
- Drug StudiesДокумент16 страницDrug Studiesvitcloud23100% (2)
- Celecoxib uses, dosage, side effectsДокумент4 страницыCelecoxib uses, dosage, side effectsAbigail LonoganОценок пока нет
- Drug Study OrthoДокумент6 страницDrug Study OrthoKrisia CastucianoОценок пока нет
- Pharm Chapter's Focus Review 2Документ16 страницPharm Chapter's Focus Review 2Briana SmetОценок пока нет
- Drug Study No.1 Brand Name: Paracetamol Generic Name: Tempra Classification: Anti-Infectives Dosage: 100mg, 1ml Drops q4hrДокумент7 страницDrug Study No.1 Brand Name: Paracetamol Generic Name: Tempra Classification: Anti-Infectives Dosage: 100mg, 1ml Drops q4hrMary EnsomoОценок пока нет
- Individual NSAIDs Mechanisms and UsesДокумент4 страницыIndividual NSAIDs Mechanisms and UsesJsnanbjrihОценок пока нет
- Bronchial Asthma 2.0Документ15 страницBronchial Asthma 2.0Bisweswar OjhaОценок пока нет
- NSAIDs, DMARDs, Analgesics & Gout DrugsДокумент114 страницNSAIDs, DMARDs, Analgesics & Gout DrugsMani Jee100% (1)
- Solu-Cortef (Hydrocortisone)Документ3 страницыSolu-Cortef (Hydrocortisone)E100% (2)
- Medical Pharmacology Ovidius 2014 1st TestДокумент19 страницMedical Pharmacology Ovidius 2014 1st TestWissam DadiОценок пока нет
- Immunology 1Документ10 страницImmunology 1Elena DalcaranОценок пока нет
- Genetics Labs 1Документ28 страницGenetics Labs 1Wissam DadiОценок пока нет
- Basic Surgical InstrumentsДокумент37 страницBasic Surgical Instrumentsapi-2658787991% (33)
- Datasheet PLASBLAK PE4637pdfДокумент2 страницыDatasheet PLASBLAK PE4637pdfGodesPow. Jose L. Godes: Entrenamiento con potenciaОценок пока нет
- Enzyme Assay Units: Amylase Units Lactase UnitsДокумент4 страницыEnzyme Assay Units: Amylase Units Lactase UnitsDaniel RincónОценок пока нет
- Hardness Desalination1Документ18 страницHardness Desalination1Swati U NaikОценок пока нет
- Rubber Property-Abrasion Resistance (Rotary Drum Abrader) : Standard Test Method ForДокумент9 страницRubber Property-Abrasion Resistance (Rotary Drum Abrader) : Standard Test Method Formohammed karasnehОценок пока нет
- Dungs ATEX en 161 Solenoid ValvesДокумент12 страницDungs ATEX en 161 Solenoid Valvesstefan-romocki-4927Оценок пока нет
- Group II Cation AnalysisДокумент4 страницыGroup II Cation AnalysisClare CaspeОценок пока нет
- Objectives Identify The Two Main Classes of Vitamins. List Seven Minerals Your Body Needs inДокумент28 страницObjectives Identify The Two Main Classes of Vitamins. List Seven Minerals Your Body Needs inyosysilalahiОценок пока нет
- Heat Transfer Study GuideДокумент6 страницHeat Transfer Study GuideCarlosCD17100% (1)
- Experiment 5Документ30 страницExperiment 5Mags CabelinОценок пока нет
- Thermal Conductivity Meter: Guarded Heat Flow Test MethodДокумент2 страницыThermal Conductivity Meter: Guarded Heat Flow Test Methodrajesh_rbpОценок пока нет
- Laboratory Manual Machine Shop 1 PDFДокумент59 страницLaboratory Manual Machine Shop 1 PDFVinz Bryan AlmacenОценок пока нет
- Lecture 1 Pendahuluan BiokatalisДокумент18 страницLecture 1 Pendahuluan BiokatalisSabar SitioОценок пока нет
- AAMA Vs Qualicoat 2018Документ12 страницAAMA Vs Qualicoat 2018viet nguyen cao0% (1)
- CentrifugationДокумент12 страницCentrifugationVytheeshwaran Vedagiri100% (16)
- Salt HydrolysisДокумент3 страницыSalt Hydrolysisna_napanda100% (1)
- Indirect RestorationsДокумент32 страницыIndirect RestorationsNaji Z. Arandi100% (1)
- Review of Literature on Aloe Vera and Hand SanitizersДокумент4 страницыReview of Literature on Aloe Vera and Hand SanitizersRamОценок пока нет
- Membrane Technology: Reverse Osmosis Ultrafiltration MicrofiltrationДокумент66 страницMembrane Technology: Reverse Osmosis Ultrafiltration MicrofiltrationShivani MunishwarОценок пока нет
- Final PG Sby 0024Документ3 страницыFinal PG Sby 0024Afwa Wildan RomadhonОценок пока нет
- Multirae Lite: Wireless Portable Multi-Gas MonitorДокумент2 страницыMultirae Lite: Wireless Portable Multi-Gas MonitorAnticristh6666Оценок пока нет
- Karbohidrat: Dyke Gita Wirasisya, S.Farm., M.SC., Apt Program Studi Farmasi, Fakultas Kedokteran, Universitas MataramДокумент37 страницKarbohidrat: Dyke Gita Wirasisya, S.Farm., M.SC., Apt Program Studi Farmasi, Fakultas Kedokteran, Universitas Matarambrahmani ptrОценок пока нет
- Acid BassДокумент41 страницаAcid BassRobert Edwards100% (1)
- 1 s2.0 S1319610311002407 MainДокумент14 страниц1 s2.0 S1319610311002407 Mainspanu oanaОценок пока нет
- Experiment 4 (Hydrates)Документ3 страницыExperiment 4 (Hydrates)Zaharahni Md SehatОценок пока нет
- Saudi Aramco Test Report: Internal Tank Bottom Testing 30-Oct-17 CP-SATR-X-3205Документ8 страницSaudi Aramco Test Report: Internal Tank Bottom Testing 30-Oct-17 CP-SATR-X-3205Tayyab AchakzaiОценок пока нет
- (Unit 1&2) PDFДокумент41 страница(Unit 1&2) PDFJaiPrakashОценок пока нет
- Evaluation of Steam Jet EjectorsДокумент11 страницEvaluation of Steam Jet EjectorsRajeh Somrani100% (3)
- Alimentos Funcionais em UanДокумент12 страницAlimentos Funcionais em UanEduardo MartinsОценок пока нет
- Who Took Jerell'S Ipod? - An Organic: Compound MysteryДокумент8 страницWho Took Jerell'S Ipod? - An Organic: Compound Mysteryakm1187Оценок пока нет
- 2010 Proportional CatalogДокумент16 страниц2010 Proportional CatalogjondesousaОценок пока нет