Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Diagram of The Tooth Numbering SystemДокумент1 страницаDiagram of The Tooth Numbering Systemsaleh900Оценок пока нет
- Central Venous Catheter (CVC) Lab Draw, Dressing Change, and Cap ChangeДокумент2 страницыCentral Venous Catheter (CVC) Lab Draw, Dressing Change, and Cap ChangePersephone Hargreeves100% (1)
- Analysis of General and Oral Quality of Life and Satisfaction With Treatment Among Anticoagulated PatientsДокумент4 страницыAnalysis of General and Oral Quality of Life and Satisfaction With Treatment Among Anticoagulated Patientslisa chanОценок пока нет
- 234 585 1 PBДокумент7 страниц234 585 1 PBlisa chanОценок пока нет
- Chapter 11 The Dental Surveyor and Its UsesДокумент4 страницыChapter 11 The Dental Surveyor and Its UsesSantosh AgarwalОценок пока нет
- Hachiko StuteДокумент6 страницHachiko Stutelisa chanОценок пока нет
- Rashid IchsanДокумент4 страницыRashid Ichsanlisa chanОценок пока нет
- Hachiko StuteДокумент6 страницHachiko Stutelisa chanОценок пока нет
- Reling Rebasing 1Документ45 страницReling Rebasing 1lisa chanОценок пока нет
- 232 570 2 PBДокумент5 страниц232 570 2 PBlisa chanОценок пока нет
- Prosthodontic DiagnosisДокумент15 страницProsthodontic DiagnosisYashpreetsingh Bhatia100% (1)
- Bleaching ReviewДокумент14 страницBleaching ReviewAbhisek DasОценок пока нет
- Hachiko StuteДокумент6 страницHachiko Stutelisa chanОценок пока нет
- Hachiko StuteДокумент6 страницHachiko Stutelisa chanОценок пока нет
- Jurnal PH PDFДокумент15 страницJurnal PH PDFason10Оценок пока нет
- Hachiko StuteДокумент6 страницHachiko Stutelisa chanОценок пока нет
- Hachiko StuteДокумент6 страницHachiko Stutelisa chanОценок пока нет
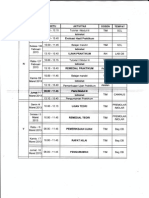
- Ikgd Blokv: Jadwal Perkuliahan TutorialДокумент1 страницаIkgd Blokv: Jadwal Perkuliahan Tutoriallisa chanОценок пока нет
- Jadwal Kuliah-Lembar 3Документ1 страницаJadwal Kuliah-Lembar 3lisa chanОценок пока нет
- Dentinogenesis: Dr. Asmat Jameel Assistant Professor B.D.S, F.C.P.S Head Department of Oral BiologyДокумент17 страницDentinogenesis: Dr. Asmat Jameel Assistant Professor B.D.S, F.C.P.S Head Department of Oral Biologylisa chanОценок пока нет
- Tugas Bahasa Inggris Nama: Lidya Kelas: XDДокумент6 страницTugas Bahasa Inggris Nama: Lidya Kelas: XDlisa chanОценок пока нет
- Hachiko StuteДокумент5 страницHachiko Stutelisa chanОценок пока нет
- Excel (Laporan Praktikum 4)Документ16 страницExcel (Laporan Praktikum 4)lisa chanОценок пока нет
- DDS FINALS Compiled ReviewerДокумент21 страницаDDS FINALS Compiled ReviewerChantelle Mea100% (1)
- CHG ChlorhexidineДокумент73 страницыCHG Chlorhexidinetaher adelОценок пока нет
- Xylitol's Role in Preventing Tooth DecayДокумент4 страницыXylitol's Role in Preventing Tooth DecayJholanda Ninggar BahtriaОценок пока нет
- Disinfection Group 3Документ21 страницаDisinfection Group 3Mosha Thadei100% (1)
- Adhesive DressingДокумент10 страницAdhesive DressingFatma ElzaytОценок пока нет
- Ebp Project Paper Summative - DeanДокумент15 страницEbp Project Paper Summative - Deanapi-252790184Оценок пока нет
- Disinfectant TypesДокумент6 страницDisinfectant TypesshrutiОценок пока нет
- Clinical and Microbial Comparative Evaluation ofДокумент5 страницClinical and Microbial Comparative Evaluation ofInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Therapeutic MouthrinsingДокумент11 страницTherapeutic MouthrinsingAmmar KizilbashОценок пока нет
- HLD SterilizationДокумент40 страницHLD Sterilizationzahisma89Оценок пока нет
- Practical Dentistry For Veterinary NursesДокумент10 страницPractical Dentistry For Veterinary NursesLucy LulubinaОценок пока нет
- Molecular Oral Microbiology - 2023 - D Amico - Efficacy of Cetylpyridinium Chloride Mouthwash Against SARS CoV 2 AДокумент10 страницMolecular Oral Microbiology - 2023 - D Amico - Efficacy of Cetylpyridinium Chloride Mouthwash Against SARS CoV 2 Akatcharles.persoОценок пока нет
- To Pack or Not To Pack: The Current Status of Periodontal DressingsДокумент14 страницTo Pack or Not To Pack: The Current Status of Periodontal DressingsJade M. LolongОценок пока нет
- Chlorhexidine For Umbilical Cord Care: Evidence Base and The Way ForwardДокумент41 страницаChlorhexidine For Umbilical Cord Care: Evidence Base and The Way ForwardsundaimeОценок пока нет
- Viskrings Seals SDSДокумент6 страницViskrings Seals SDSTarik ConceptОценок пока нет
- Antimicrobial effects of endodontic irrigants on microorganismsДокумент4 страницыAntimicrobial effects of endodontic irrigants on microorganismsAna Cernaianu0% (1)
- Yash PaulДокумент8 страницYash Paulal rzОценок пока нет
- Title Page: MISS NORMALIZA AM AB MALIK (Orcid ID: 0000-0002-0423-0837)Документ23 страницыTitle Page: MISS NORMALIZA AM AB MALIK (Orcid ID: 0000-0002-0423-0837)dwiwahyu ningsihОценок пока нет
- GMMMG Dental Prescribing Guidelines February 2020 v1 0Документ4 страницыGMMMG Dental Prescribing Guidelines February 2020 v1 0Erick GuanoluisaОценок пока нет
- A Review of Chlorhexidine and Its Use in Special PopulationsДокумент7 страницA Review of Chlorhexidine and Its Use in Special PopulationseliasberniОценок пока нет
- Antibacterial and Antifungal Drugs: Department of Chemistry University of HullДокумент60 страницAntibacterial and Antifungal Drugs: Department of Chemistry University of HullIrawan RiyanОценок пока нет
- 2010 - Octenidine Dihydrochloride, A Modern Antiseptic For Skin, Mucous Membranes and WoundsДокумент15 страниц2010 - Octenidine Dihydrochloride, A Modern Antiseptic For Skin, Mucous Membranes and Woundsnovia100% (2)
- HH - DR FrankaДокумент25 страницHH - DR FrankaHannan AliОценок пока нет
- How Does Oracort WorkДокумент4 страницыHow Does Oracort WorkAnonymous G8oZXHJrОценок пока нет
- Dr. Hayder Hamed Abed B.Sc. M.Sc. PH.D.: Key Word: Stability Study-Long Term - Chlorhexidine GluconateДокумент8 страницDr. Hayder Hamed Abed B.Sc. M.Sc. PH.D.: Key Word: Stability Study-Long Term - Chlorhexidine GluconateMạnh CườngОценок пока нет
- Chemical Plaque Control Agents GuideДокумент44 страницыChemical Plaque Control Agents GuideMahnoor MustafaОценок пока нет
- Antiseptics & DisinfectantsДокумент33 страницыAntiseptics & DisinfectantsChoice OrganoОценок пока нет
- Synthesis, Characterization, and Antimicrobial Investigation of A Novel Chlorhexidine Cyclamate ComplexДокумент25 страницSynthesis, Characterization, and Antimicrobial Investigation of A Novel Chlorhexidine Cyclamate ComplexGalileu E TamyОценок пока нет
- Irrigation in EndodonticsДокумент94 страницыIrrigation in EndodonticsRajsandeep SinghОценок пока нет