Вам также может понравиться
- Practical Gastroenterology and Hepatology Board Review ToolkitОт EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultОценок пока нет
- First Aid PsychiatryДокумент156 страницFirst Aid PsychiatryMae Matira AbeladorОценок пока нет
- 200 PSM Questions Solved by DR AshwaniДокумент16 страниц200 PSM Questions Solved by DR AshwaniShaaron Sky SonaОценок пока нет
- Oncology Questions by DR - OkashaДокумент31 страницаOncology Questions by DR - Okashamohammed okashaОценок пока нет
- OSPE 4th Yr PathoДокумент144 страницыOSPE 4th Yr PathoMuhammadShahzadОценок пока нет
- Evidence Based Medicine Beginners HandbookДокумент40 страницEvidence Based Medicine Beginners HandbookcmegmhiОценок пока нет
- Thyroid NodulesДокумент34 страницыThyroid NodulesEphobiaОценок пока нет
- PSM 2nd With AnswerДокумент24 страницыPSM 2nd With AnswerAshiq Syedali PichiVilaakamОценок пока нет
- Thesis of Dr. AKM Maruf Raza PDFДокумент95 страницThesis of Dr. AKM Maruf Raza PDFMaruf Raza DarubagiОценок пока нет
- MBChB4 5PastPapersДокумент172 страницыMBChB4 5PastPapersHariharan NarendranОценок пока нет
- Drug Toxicity and PoisoningДокумент12 страницDrug Toxicity and PoisoningPAULA MARIE MERCADO LLIDOОценок пока нет
- Obs and Gyn Past Paper AnswersДокумент15 страницObs and Gyn Past Paper AnswersJunYuuuОценок пока нет
- Evidence Based Medicine (UTI)Документ20 страницEvidence Based Medicine (UTI)Migs ValdezОценок пока нет
- Important QuestionsДокумент31 страницаImportant QuestionssandeepОценок пока нет
- Matary Differential Diagnosis 2013 PDFДокумент128 страницMatary Differential Diagnosis 2013 PDFAlejandra Rozo BayerОценок пока нет
- Sample Surgery QuestionsДокумент98 страницSample Surgery QuestionspandaОценок пока нет
- اسئله جراحه عامه سنوات سابقه امتحان الامتيازДокумент110 страницاسئله جراحه عامه سنوات سابقه امتحان الامتيازZaid Zayed100% (1)
- Bethesda ScoreДокумент7 страницBethesda ScoreTiberiu BircaОценок пока нет
- Pathology Mcq's - XenoMEDДокумент11 страницPathology Mcq's - XenoMEDfreeuser3Оценок пока нет
- DR Ashiq Tutorials Pre-Krok 1222Документ66 страницDR Ashiq Tutorials Pre-Krok 1222Praveen KpОценок пока нет
- Internal Medicine 5th MidtermДокумент13 страницInternal Medicine 5th MidtermIashdip iashdipОценок пока нет
- Mid QuestionsДокумент4 страницыMid QuestionsMAMA LALAОценок пока нет
- Summer 2016 MCQДокумент16 страницSummer 2016 MCQDaniel CoyleОценок пока нет
- Surgery History and PhysicalДокумент23 страницыSurgery History and PhysicalBilal RowaihiОценок пока нет
- Transplantation: Presented by Santhiya K II M.SC Biotechnology 18PBT014Документ54 страницыTransplantation: Presented by Santhiya K II M.SC Biotechnology 18PBT014AbiОценок пока нет
- Pathology Question BankДокумент9 страницPathology Question BankShaimaa AbabnehОценок пока нет
- Community MedicineДокумент77 страницCommunity MedicineSharon DanielОценок пока нет
- Carcinoma of The Breast - Bailey & LoveДокумент5 страницCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- Pathology Questions PDFДокумент67 страницPathology Questions PDFDhruva PatelОценок пока нет
- SurgeryДокумент14 страницSurgeryVinit ChoudharyОценок пока нет
- Chapter 1. History and Physical Examination - Art and ScienceДокумент3 страницыChapter 1. History and Physical Examination - Art and SciencecarolineОценок пока нет
- Bates Outline of Chapter 8Документ15 страницBates Outline of Chapter 8KatherynSotoОценок пока нет
- Gyne ObsqsДокумент30 страницGyne ObsqsMarsFriendОценок пока нет
- Systemic Response To InjuryДокумент58 страницSystemic Response To InjuryJustinОценок пока нет
- H&P GuideДокумент7 страницH&P GuideTBWPОценок пока нет
- Hepatobiliary ExamДокумент10 страницHepatobiliary ExamAllison Eunice Servando100% (1)
- Pro 1213 MCQ 2Документ15 страницPro 1213 MCQ 2Jabraan JamilОценок пока нет
- Chapterwise Question Bank-1Документ188 страницChapterwise Question Bank-1msreyaОценок пока нет
- Liver Pathology EMQДокумент1 страницаLiver Pathology EMQhazirmm100% (2)
- Kod - S Guide On Final Professional Exam 1 PDFДокумент31 страницаKod - S Guide On Final Professional Exam 1 PDFHassanAbasОценок пока нет
- Breast Disorder: by DR - Wael MetwalyДокумент7 страницBreast Disorder: by DR - Wael MetwalyhasebeОценок пока нет
- FBC Interpretation and Function of Blood ComponentsДокумент7 страницFBC Interpretation and Function of Blood ComponentsFrancesca LiОценок пока нет
- Cardiology PDFДокумент27 страницCardiology PDFNada AKОценок пока нет
- The Post Splenectomy Blood PDFДокумент2 страницыThe Post Splenectomy Blood PDFnaftalina7Оценок пока нет
- Oral Boards 2Документ67 страницOral Boards 2Steven GodelmanОценок пока нет
- Diagnostic Liver Biopsy PDFДокумент7 страницDiagnostic Liver Biopsy PDFAriadna MarielОценок пока нет
- Sem 4 MCQ Week 4 Jan 2014 CTL McqsДокумент15 страницSem 4 MCQ Week 4 Jan 2014 CTL McqsFlowerОценок пока нет
- Interpretation of CBCДокумент35 страницInterpretation of CBCnth1992Оценок пока нет
- NemaoДокумент94 страницыNemaoRoxenette Gil Bernales PangilinanОценок пока нет
- Uworld GI NotesДокумент17 страницUworld GI NotesAyodeji SotimehinОценок пока нет
- Ophelia'S Case: Oleh: Anggun Fitri Utami, S, Ked PembimbingДокумент20 страницOphelia'S Case: Oleh: Anggun Fitri Utami, S, Ked PembimbingAnggun Cimey UtamiОценок пока нет
- L12 Shock MCQ'sДокумент4 страницыL12 Shock MCQ'srida hafeezОценок пока нет
- Pancoast TumorДокумент26 страницPancoast TumorDhanis HastinОценок пока нет
- Usmle QuestionsДокумент18 страницUsmle QuestionsPat FelleОценок пока нет
- Internal MedicineДокумент161 страницаInternal Medicinemain.genevive.dilig100% (1)
- Major Tropical Diseases - Prof. Dr. Sugeng JuwonoДокумент48 страницMajor Tropical Diseases - Prof. Dr. Sugeng JuwonosittihajarОценок пока нет
- SpleenДокумент7 страницSpleenAkinniyi100% (1)
- PheochromocytomaДокумент30 страницPheochromocytomaMirza Yousuf Baig100% (1)
- Van de Graaff GeneratorДокумент10 страницVan de Graaff GeneratorJihad AnadОценок пока нет
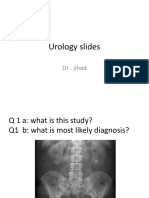
- Urology Slides: DR - JihadДокумент4 страницыUrology Slides: DR - JihadJihad Anad100% (1)
- Irrigating Fluids in Endoscopic Surgery: ReviewДокумент12 страницIrrigating Fluids in Endoscopic Surgery: ReviewJihad AnadОценок пока нет
- Uro SepsisДокумент23 страницыUro SepsisJihad Anad100% (1)
- Urology Slides: DR - JihadДокумент4 страницыUrology Slides: DR - JihadJihad Anad100% (1)
- Ultrasound NotesДокумент19 страницUltrasound NotesJihad Anad100% (1)
- JSCFE Guidance Notes For Applicants - GenericДокумент2 страницыJSCFE Guidance Notes For Applicants - GenericJihad AnadОценок пока нет
- Penile Prosthesis Implantation in Chinese Patients With Severe Erectile Dysfunction: 10-Year ExperienceДокумент4 страницыPenile Prosthesis Implantation in Chinese Patients With Severe Erectile Dysfunction: 10-Year ExperienceJihad AnadОценок пока нет
- JSCFE Guidance Notes For Referees - GenericДокумент2 страницыJSCFE Guidance Notes For Referees - GenericJihad AnadОценок пока нет
- Aleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Документ14 страницAleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Jihad AnadОценок пока нет
- Answer For Urology MCQДокумент1 страницаAnswer For Urology MCQJihad AnadОценок пока нет
- Antibiotics: by Dr. Jihad AnadДокумент89 страницAntibiotics: by Dr. Jihad AnadJihad AnadОценок пока нет
- Urology OSCEДокумент9 страницUrology OSCEJihad Anad75% (4)
- DiureticsДокумент6 страницDiureticsJihad AnadОценок пока нет
- AbstractДокумент2 страницыAbstractJihad AnadОценок пока нет
- 500 Mcqs Surgery and RadiologyДокумент66 страниц500 Mcqs Surgery and RadiologyJihad Anad81% (59)
- ChoeДокумент116 страницChoeJihad AnadОценок пока нет
- Appendix E: Microsoft Excel 2010 and Tools For Statistical AnalysisДокумент15 страницAppendix E: Microsoft Excel 2010 and Tools For Statistical AnalysisJihad AnadОценок пока нет
- MCQ RadiologyДокумент10 страницMCQ RadiologyJihad Anad100% (2)
- Success With Penile Prosthesis From Patient'S ViewpointДокумент3 страницыSuccess With Penile Prosthesis From Patient'S ViewpointJihad AnadОценок пока нет
- Urology PDFДокумент188 страницUrology PDFAmr BashaОценок пока нет
- Care of Clients With Problems of The Male Reproductive SystemДокумент18 страницCare of Clients With Problems of The Male Reproductive SystemwakswafuОценок пока нет
- Multiple Choice Questions For Urinary Obstruction and BPH: E. Too Much Urine Produced by The KidneyДокумент3 страницыMultiple Choice Questions For Urinary Obstruction and BPH: E. Too Much Urine Produced by The KidneyOe MahardikaОценок пока нет
- STRING v9.1: Edges and Nodes Provide Global Functional Association To Protein Crosstalk and Integration in Urinary Proteomes of Prostate CancerДокумент3 страницыSTRING v9.1: Edges and Nodes Provide Global Functional Association To Protein Crosstalk and Integration in Urinary Proteomes of Prostate CancerNora AutusОценок пока нет
- Pathophysiology BPH Case StudyДокумент3 страницыPathophysiology BPH Case Studyyhanne100% (24)
- BPH and HematuriaДокумент40 страницBPH and HematuriaJohn LeeОценок пока нет
- To Study The Necessity of Clamping Versus Non Clamping in Short Duration Urinary Catheter Removal in Operated Orthopaedic PatientsДокумент4 страницыTo Study The Necessity of Clamping Versus Non Clamping in Short Duration Urinary Catheter Removal in Operated Orthopaedic PatientsIJAR JOURNALОценок пока нет
- 12 Best Natural DHT BlockersДокумент16 страниц12 Best Natural DHT Blockersstummel6636Оценок пока нет
- Urology Questions Bank PDFДокумент16 страницUrology Questions Bank PDFPalwasha Malik40% (5)
- Primary and Secondary Prevention of Benign Prostatic HyperplasiaДокумент2 страницыPrimary and Secondary Prevention of Benign Prostatic HyperplasiaNina MelinaОценок пока нет
- Challenging PDGM Coding ScenariosДокумент41 страницаChallenging PDGM Coding ScenariosLaluMohan KcОценок пока нет
- CVMU Market OverviewДокумент10 страницCVMU Market OverviewAzfar NiyaziОценок пока нет
- Tamsulosin and The Risk of Dementia in Older Men With BenignДокумент9 страницTamsulosin and The Risk of Dementia in Older Men With BenignTerra PapelОценок пока нет
- Alterations in Urinary EliminationДокумент76 страницAlterations in Urinary EliminationJenny Tran75% (4)
- Desenvolviemento de Formulação - NatestoДокумент24 страницыDesenvolviemento de Formulação - NatestoIrma pedroОценок пока нет
- Postobstructive Diuresis: Clinical ReviewДокумент6 страницPostobstructive Diuresis: Clinical ReviewRara Aulia IIОценок пока нет
- Etiology, Epidemiology, and Natural History HBPДокумент13 страницEtiology, Epidemiology, and Natural History HBPuricoletОценок пока нет
- Mono - Pygeum Prunus Africana - EnglishДокумент5 страницMono - Pygeum Prunus Africana - EnglishTom DelongeОценок пока нет
- Guidlines BPHДокумент64 страницыGuidlines BPHArusyha ZhafiraОценок пока нет
- Aapc 2016Документ92 страницыAapc 2016Ravi Pal75% (4)
- PNSG 214 Drug Research Assignment 2022 NewДокумент14 страницPNSG 214 Drug Research Assignment 2022 Newapi-596613382Оценок пока нет
- Medical Term PQRSTДокумент37 страницMedical Term PQRSTTika Arizon R NОценок пока нет
- Biology THE RENAL SYSTEM OutputДокумент7 страницBiology THE RENAL SYSTEM OutputRhea CabillaОценок пока нет
- BPH and VesikolithiasisДокумент22 страницыBPH and VesikolithiasisPutri Dwi Kartini0% (1)
- LUTS Assessment LURN Symptom IndexДокумент17 страницLUTS Assessment LURN Symptom IndexOmar Salim AkhtarОценок пока нет
- Nbme 5.1Документ54 страницыNbme 5.1Hafsa SafdarОценок пока нет
- Prevalence of Lower Urinary Tract Symptoms in Austria As Assessed by An Open Survey of 2,096 MenДокумент6 страницPrevalence of Lower Urinary Tract Symptoms in Austria As Assessed by An Open Survey of 2,096 MenBandac AlexandraОценок пока нет
- WWW Drleena Co in 10 Most Common Causes of Pelvic Pain in Men HTMLДокумент2 страницыWWW Drleena Co in 10 Most Common Causes of Pelvic Pain in Men HTMLtylermcgrath12546Оценок пока нет
- Genitourinary ObjectivesДокумент38 страницGenitourinary Objectivescwumspa14Оценок пока нет
- Beitz 2014Документ10 страницBeitz 2014Anna Beatriz Silva EspindolaОценок пока нет
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 4.5 из 5 звезд4.5/5 (82)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (254)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (60)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisОт EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisРейтинг: 5 из 5 звезд5/5 (8)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (5)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedРейтинг: 4 из 5 звезд4/5 (61)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (46)