Вам также может понравиться
- Human Brain in Standard MNI Space: A Comprehensive Pocket AtlasОт EverandHuman Brain in Standard MNI Space: A Comprehensive Pocket AtlasОценок пока нет
- Temporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTДокумент6 страницTemporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTNovi DwiyantiОценок пока нет
- Segmentation of Brain Tissue From Magnetic Resonance ImagesДокумент42 страницыSegmentation of Brain Tissue From Magnetic Resonance Imageshub23Оценок пока нет
- JARVIS ProjectДокумент39 страницJARVIS ProjectThirupathyОценок пока нет
- Mricro CostДокумент10 страницMricro CostToon ManОценок пока нет
- Statistical Parametric Mapping: The Analysis of Functional Brain ImagesОт EverandStatistical Parametric Mapping: The Analysis of Functional Brain ImagesРейтинг: 4.5 из 5 звезд4.5/5 (2)
- Segmentation of Brain Structures in Presence of A Space-Occupying LesionДокумент7 страницSegmentation of Brain Structures in Presence of A Space-Occupying LesionzuhirdaОценок пока нет
- Totalsegmentator: Robust Segmentation of 104 Anatomical Structures in CT ImagesДокумент44 страницыTotalsegmentator: Robust Segmentation of 104 Anatomical Structures in CT ImagesanhtainguyenluuОценок пока нет
- Fluorescence Microscopy: Super-Resolution and other Novel TechniquesОт EverandFluorescence Microscopy: Super-Resolution and other Novel TechniquesAnda CorneaОценок пока нет
- 3 PDFДокумент6 страниц3 PDFchetanajitesh76Оценок пока нет
- Eng-Cyst Detection in MRI Brain Image-Vrushali D. DharmaleДокумент10 страницEng-Cyst Detection in MRI Brain Image-Vrushali D. DharmaleImpact JournalsОценок пока нет
- A Reference Dataset For Verifying Numerical Electrophysiological Heart ModelsДокумент15 страницA Reference Dataset For Verifying Numerical Electrophysiological Heart ModelsBikerz ChopperОценок пока нет
- Classifying Brain Tumors Using Wavelet Texture FeaturesДокумент10 страницClassifying Brain Tumors Using Wavelet Texture FeaturesbelajartvkuОценок пока нет
- Tomography ThesisДокумент7 страницTomography ThesisApril Smith100% (2)
- Sadeghi Goughari2016Документ17 страницSadeghi Goughari2016Petra Banda RamirezОценок пока нет
- ReportДокумент18 страницReportEshwarОценок пока нет
- Features: Medical Image RegistrationДокумент4 страницыFeatures: Medical Image RegistrationWill SmithОценок пока нет
- Deep Learning Methods To Generate Synthetic CT From MRI in Radiotherapy A Literature ReviewДокумент17 страницDeep Learning Methods To Generate Synthetic CT From MRI in Radiotherapy A Literature ReviewColman SiuОценок пока нет
- Automatic Classification of Alzheimer's Disease Using Brain MRI Data and Deep Convolutional Neural NetworksДокумент27 страницAutomatic Classification of Alzheimer's Disease Using Brain MRI Data and Deep Convolutional Neural NetworksRereyОценок пока нет
- Ultrasound Imaging ThesisДокумент7 страницUltrasound Imaging Thesisbrendazerrindependence100% (2)
- Image Fusion For Conformal Radiation TherapyДокумент13 страницImage Fusion For Conformal Radiation TherapyAntonio López MedinaОценок пока нет
- Med Img Brain SegДокумент19 страницMed Img Brain SegThalib MirzaОценок пока нет
- The Computer Journal 2009 Greenspan 43 63Документ21 страницаThe Computer Journal 2009 Greenspan 43 63A. D. PrasadОценок пока нет
- Brain Stroke Computed Tomography Images Analysis Using Image Processing: A ReviewДокумент12 страницBrain Stroke Computed Tomography Images Analysis Using Image Processing: A ReviewIAES IJAIОценок пока нет
- Modeling Human Tissues with Image SegmentationДокумент28 страницModeling Human Tissues with Image SegmentationAnonymous 6WeX00mx0Оценок пока нет
- 20026Документ7 страниц20026zelvininaprilia990Оценок пока нет
- Karnan and LogeswariДокумент9 страницKarnan and LogeswariPrasanna ThiОценок пока нет
- Comunicacion 0 1367916178633 PDFДокумент4 страницыComunicacion 0 1367916178633 PDFdominlopezОценок пока нет
- Siemens Healthineers Magnetom Flash 71 MR Spectroscopy in Neuroimaging Ryner 1800000005860250Документ10 страницSiemens Healthineers Magnetom Flash 71 MR Spectroscopy in Neuroimaging Ryner 1800000005860250Ana Sofia PintoОценок пока нет
- VIRTOPSY The Swiss Virtual Autopsy ApproachДокумент5 страницVIRTOPSY The Swiss Virtual Autopsy ApproachgarethОценок пока нет
- Transfer Learning Based Deep Learning Framework For Identification of Type of Brain TumorДокумент6 страницTransfer Learning Based Deep Learning Framework For Identification of Type of Brain TumorTole SutiknoОценок пока нет
- Unesco97Документ21 страницаUnesco97Leonell Romero BazanОценок пока нет
- MRI-Based Attenuation Correction For PET/MRI Using Ultrashort Echo Time SequencesДокумент8 страницMRI-Based Attenuation Correction For PET/MRI Using Ultrashort Echo Time SequencesOmarah AbdalqaderОценок пока нет
- Main PDFДокумент8 страницMain PDFnadeemq_0786Оценок пока нет
- Survey On Diagnosis of Brain Hemorrhage by Using Artificial Neural NetworkДокумент4 страницыSurvey On Diagnosis of Brain Hemorrhage by Using Artificial Neural NetworkijsretОценок пока нет
- DiagnosticsДокумент4 страницыDiagnosticsfrancimaria02Оценок пока нет
- Detect Tumour in 3D Brain MRI Using K-Means ClusteringДокумент6 страницDetect Tumour in 3D Brain MRI Using K-Means ClusteringJeevan KishorОценок пока нет
- Applied Sciences: Classification of Brain Tumors From MRI Images Using A Convolutional Neural NetworkДокумент13 страницApplied Sciences: Classification of Brain Tumors From MRI Images Using A Convolutional Neural NetworkZe PushОценок пока нет
- Neuroimage: Contents Lists Available atДокумент18 страницNeuroimage: Contents Lists Available atWinda HidayatiОценок пока нет
- Improved Accuracy of Brain Tumor Detection Using VGG16Документ9 страницImproved Accuracy of Brain Tumor Detection Using VGG16IJRASETPublicationsОценок пока нет
- Applied Sciences: Deep Learning-Based Automatic Segmentation of Mandible and Maxilla in Multi-Center CT ImagesДокумент15 страницApplied Sciences: Deep Learning-Based Automatic Segmentation of Mandible and Maxilla in Multi-Center CT ImagesDyah Dhani MustikariniОценок пока нет
- JPM 10 00224 v3Документ27 страницJPM 10 00224 v3thouraya hadj hassenОценок пока нет
- MRI en RadioterapiaДокумент19 страницMRI en Radioterapia980Denis FernandezОценок пока нет
- Interpretasi CT ScanДокумент19 страницInterpretasi CT ScanAB KristiadiОценок пока нет
- Gambar Slowctlewis2009Документ12 страницGambar Slowctlewis2009Andreas RonaldОценок пока нет
- A New Method of MRI Examination For The Sternoclavicular JointsДокумент12 страницA New Method of MRI Examination For The Sternoclavicular JointsRafael CamposОценок пока нет
- Dissertation MriДокумент7 страницDissertation MriEnglishPaperHelpSingapore100% (1)
- T2 NanthagopalДокумент10 страницT2 Nanthagopaladin80Оценок пока нет
- Computed Tomography and Magnetic Resonance ImagingДокумент14 страницComputed Tomography and Magnetic Resonance ImagingChecko LatteОценок пока нет
- Hybrid Model Implementation For Brain Tumor Detection System Using Deep Neural NetworksДокумент8 страницHybrid Model Implementation For Brain Tumor Detection System Using Deep Neural NetworksIJRASETPublicationsОценок пока нет
- Diagnostics 11 01589 v2Документ19 страницDiagnostics 11 01589 v2sekharraoОценок пока нет
- Brain Tumor Segmentation ThesisДокумент7 страницBrain Tumor Segmentation Thesisafksooisybobce100% (2)
- Diffuse Optical Tomography ThesisДокумент6 страницDiffuse Optical Tomography Thesisbk1hxs86100% (2)
- 56Документ5 страниц56Jawwad SamiОценок пока нет
- An Efficient Visualization and Segmentation of Lung CT Scan Images For Early Diagnosis of CancerДокумент5 страницAn Efficient Visualization and Segmentation of Lung CT Scan Images For Early Diagnosis of Cancermaruthi631Оценок пока нет
- DownloadДокумент9 страницDownloadhasan nazzalОценок пока нет
- Bhcs Maths Roadmap 2019Документ1 страницаBhcs Maths Roadmap 2019Michael100% (1)
- Transforming Translational Research: Bridging The GapДокумент2 страницыTransforming Translational Research: Bridging The GapMichaelОценок пока нет
- Lee 2006Документ13 страницLee 2006MichaelОценок пока нет
- STparamsДокумент1 страницаSTparamsMichaelОценок пока нет
- Moyamoya DiseaseДокумент12 страницMoyamoya DiseaseFarida Irawati SiregarОценок пока нет
- Liquid-Cooling by LairdДокумент6 страницLiquid-Cooling by LairdAman SinghОценок пока нет
- CQ X-Ray CT Film QualityДокумент43 страницыCQ X-Ray CT Film QualityAlfonso NiñoОценок пока нет
- CEFALEA Evaluation of Headache in Adults - UpToDateДокумент23 страницыCEFALEA Evaluation of Headache in Adults - UpToDateJOSE ANTONIO ALBARRAN MENDOZAОценок пока нет
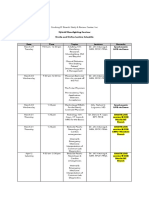
- Hybrid Moonlighting Seminar ScheduleДокумент2 страницыHybrid Moonlighting Seminar ScheduleSanielle Karla Garcia LorenzoОценок пока нет
- ZULVA The Incidence and Outcome of Major Complication TAE TACEДокумент6 страницZULVA The Incidence and Outcome of Major Complication TAE TACERSU DUTA MULYAОценок пока нет
- 3D Treatment Planning in Head & NeckДокумент29 страниц3D Treatment Planning in Head & NeckErick Natividad Zevallos0% (1)
- صيانة الاجهزة والمعدات الطبيةДокумент83 страницыصيانة الاجهزة والمعدات الطبيةSayed BadawyОценок пока нет
- Vivid S5 Data SheetДокумент10 страницVivid S5 Data Sheetmuhammed kalet100% (1)
- Brain Tumor Segmentation by K.Muthu Kumar, PSN CollegeДокумент7 страницBrain Tumor Segmentation by K.Muthu Kumar, PSN Collegeமுத்து குமார்Оценок пока нет
- CT Basic Principle & CT NumberДокумент30 страницCT Basic Principle & CT NumberAtri thakerОценок пока нет
- Acta 88 96Документ11 страницActa 88 96Santosh KumarОценок пока нет
- Diagrams For X-Series MonitorДокумент7 страницDiagrams For X-Series MonitorRashid Kh100% (1)
- Naspub Muhammad IzzudinДокумент15 страницNaspub Muhammad IzzudinMuhammad IzzudinОценок пока нет
- Console Advance Brochure EnglishДокумент5 страницConsole Advance Brochure Englishlabel engineering companyОценок пока нет
- IEEE Recommended Practice For Establishing Transformer Capability When Supplying Nonsinusoidal Load CurrentsДокумент15 страницIEEE Recommended Practice For Establishing Transformer Capability When Supplying Nonsinusoidal Load CurrentsNicolásColomberoОценок пока нет
- Transcranial Magnetic Stimulation - A Neurochronometrics of MindДокумент322 страницыTranscranial Magnetic Stimulation - A Neurochronometrics of MindMrSelleck100% (1)
- Confocal Microwave Imaging For Breast Cancer Detection Delay-Multiply-and-Sum Image Reconstruction AlgorithmДокумент8 страницConfocal Microwave Imaging For Breast Cancer Detection Delay-Multiply-and-Sum Image Reconstruction Algorithmİsmail İlke GüngörОценок пока нет
- Radiology Department Strategies To Protect RadioloДокумент5 страницRadiology Department Strategies To Protect RadioloeugeniaОценок пока нет
- KCR 2019 Abstract Book-SE - NeuroradiologyДокумент66 страницKCR 2019 Abstract Book-SE - NeuroradiologyJANBADE PURVESH ATUL (PGP 2016-18)Оценок пока нет
- Systematic Review - Cardiac LipomaДокумент7 страницSystematic Review - Cardiac LipomaEspecialização EcocardiografiaОценок пока нет
- StudentHandbookEE200 PDFДокумент34 страницыStudentHandbookEE200 PDFboshi moroboshiОценок пока нет
- Brochure Fabius MRIДокумент10 страницBrochure Fabius MRILil_QuinceОценок пока нет
- Nexus - Harry Oldfield PDFДокумент7 страницNexus - Harry Oldfield PDFDonatMaglić100% (1)
- Siemens SOMATOM ForceДокумент66 страницSiemens SOMATOM ForceNgọc Hoàng TuấnОценок пока нет
- Example of SPMPДокумент7 страницExample of SPMPRoberto Julianto KondoruraОценок пока нет
- Acute Onset Flank Pain PDFДокумент6 страницAcute Onset Flank Pain PDFYuliana WiralestariОценок пока нет
- Ultrasonic Sampling Phased Array Testing As A Replacement For X-Ray Testing of Weld Joints in Ship ConstructionДокумент4 страницыUltrasonic Sampling Phased Array Testing As A Replacement For X-Ray Testing of Weld Joints in Ship ConstructionRiza KhanОценок пока нет
- Metlife Bangladesh Lifecard Discount ProvidersДокумент17 страницMetlife Bangladesh Lifecard Discount ProvidersABDUL ALIM75% (4)
- Basic Radiation OncologyДокумент587 страницBasic Radiation OncologyMedCR1987Оценок пока нет
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (18)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosОт Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosРейтинг: 4.5 из 5 звезд4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОценок пока нет
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingОт EverandThe Happiness Trap: How to Stop Struggling and Start LivingРейтинг: 4 из 5 звезд4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsОт EverandAlgorithms to Live By: The Computer Science of Human DecisionsРейтинг: 4.5 из 5 звезд4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedРейтинг: 4 из 5 звезд4/5 (11)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Secure Love: Create a Relationship That Lasts a LifetimeОт EverandSecure Love: Create a Relationship That Lasts a LifetimeРейтинг: 5 из 5 звезд5/5 (18)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)