Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- KadДокумент25 страницKadraisaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Syok KardiogenikДокумент31 страницаSyok KardiogenikcantikarevieraОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- P Knowlesi PDFДокумент3 страницыP Knowlesi PDFNurbieber Saiianklylavrilavigne BieberОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Osteoporosis F DHДокумент39 страницOsteoporosis F DH95kodok85Оценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Telmisartan AmlodipineДокумент10 страницTelmisartan AmlodipineDeby Tri Widia LestariОценок пока нет
- HonkДокумент11 страницHonkYozhanОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Disease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdДокумент57 страницDisease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDeby Tri Widia LestariОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- GPQ 20 Jun08 PDFДокумент4 страницыGPQ 20 Jun08 PDFDeby Tri Widia LestariОценок пока нет
- Kuliah Obat Esensial Dan FormulariumДокумент12 страницKuliah Obat Esensial Dan FormulariumNita RahmatunnisaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Japan Earthquake HighlightedДокумент3 страницыJapan Earthquake HighlightedDeby Tri Widia LestariОценок пока нет
- 0704 06Документ4 страницы0704 06Deby Tri Widia LestariОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Konsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarДокумент4 страницыKonsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarTegoeh RizkiОценок пока нет
- Sexual Violence Sept 2014 152Документ6 страницSexual Violence Sept 2014 152Deby Tri Widia LestariОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Headache QuestionnaireДокумент10 страницHeadache QuestionnairePerisha VeeraОценок пока нет
- 15Документ5 страниц15Deby Tri Widia LestariОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
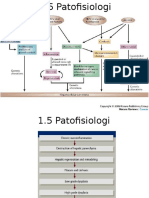
- 1.5 Patofisiologi Karsinoma HepatoselulerДокумент2 страницы1.5 Patofisiologi Karsinoma HepatoselulerDeby Tri Widia LestariОценок пока нет
- NAP For Web - Headache Diagnosis TestingДокумент38 страницNAP For Web - Headache Diagnosis TestingDeby Tri Widia LestariОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- VaksinasiДокумент9 страницVaksinasiDeby Tri Widia LestariОценок пока нет
- Migraine Prevalence, Alexithymia, and Post-Traumatic StressДокумент9 страницMigraine Prevalence, Alexithymia, and Post-Traumatic StressDeby Tri Widia LestariОценок пока нет
- IndianJMedSci6611-3703196 101711Документ12 страницIndianJMedSci6611-3703196 10171195kodok85Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Life Stress TestДокумент2 страницыLife Stress Test95kodok85Оценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Stress Dan AnxietasДокумент4 страницыStress Dan AnxietasIhsan Rasyid YuldiОценок пока нет
- Prevalence of Stress Among Medical Students in Jizan University Kingdom of Saudi ArabiaДокумент7 страницPrevalence of Stress Among Medical Students in Jizan University Kingdom of Saudi ArabiaDeby Tri Widia LestariОценок пока нет
- Epidemiological Investigation of A Temporal Increase in Atonic Postpartum Haemorrhage A Population-Based Retrospective Cohort StudyДокумент10 страницEpidemiological Investigation of A Temporal Increase in Atonic Postpartum Haemorrhage A Population-Based Retrospective Cohort StudyDeby Tri Widia LestariОценок пока нет
- Maternal Near Miss in Rural Hospital SudanДокумент4 страницыMaternal Near Miss in Rural Hospital SudanVikas LonikarОценок пока нет
- Konsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarДокумент4 страницыKonsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarTegoeh RizkiОценок пока нет
- Prevalence of Anemia Risk Factors in Pregnant Women in Kerman, IranДокумент4 страницыPrevalence of Anemia Risk Factors in Pregnant Women in Kerman, IranDeby Tri Widia LestariОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Exsanguinated Uterus After Massive Atonic Postpartum HaemorrhageДокумент4 страницыExsanguinated Uterus After Massive Atonic Postpartum HaemorrhageDeby Tri Widia LestariОценок пока нет
- Postpartum Haemorrhage in Midwifery Care in The Netherlands Validation of Quality Indicators For Midwifery GuidelinesДокумент6 страницPostpartum Haemorrhage in Midwifery Care in The Netherlands Validation of Quality Indicators For Midwifery GuidelinesDeby Tri Widia LestariОценок пока нет