Вам также может понравиться
- TREATMENT OF 71 YEAR OLD GRANNY WITH STAGE II HYPERTENSION AND HYPERCHOLESTEROLEMIAДокумент13 страницTREATMENT OF 71 YEAR OLD GRANNY WITH STAGE II HYPERTENSION AND HYPERCHOLESTEROLEMIAagathaaveonitaОценок пока нет
- Case Report ScabiesДокумент28 страницCase Report ScabiesPattiyahalatasОценок пока нет
- 13 - 266fourniers Gangrene PDFДокумент5 страниц13 - 266fourniers Gangrene PDFMochamad RizalОценок пока нет
- Journal ReadingДокумент18 страницJournal ReadingnafisyarifahОценок пока нет
- Radiologis Gambaran Infeksi Tulang dan FrakturДокумент25 страницRadiologis Gambaran Infeksi Tulang dan FrakturAnonymous HAbhRTs2TfОценок пока нет
- Case Report Omsk Brian JoviДокумент16 страницCase Report Omsk Brian Joviaisyah18Оценок пока нет
- Blok-22-Meningitis-Tuberkulosis Fakhrurrozi PratamaДокумент16 страницBlok-22-Meningitis-Tuberkulosis Fakhrurrozi PratamaFakhrurrozi PratamaОценок пока нет
- Otitis Media AkutДокумент31 страницаOtitis Media AkutNin DuskОценок пока нет
- Syphilis CongenitalДокумент5 страницSyphilis CongenitalElisse StephanieОценок пока нет
- REFERAT Cluster HeadacheДокумент39 страницREFERAT Cluster HeadacheSafitriОценок пока нет
- Guildelines For Hiv Testing NacoДокумент165 страницGuildelines For Hiv Testing NacoNagendra Singh BeniwalОценок пока нет
- Journal Reading THT - OMAДокумент15 страницJournal Reading THT - OMAIndira MaycellaОценок пока нет
- Anatomi, Eflouresensi KulitДокумент67 страницAnatomi, Eflouresensi KulitWhydia Wedha SutedjaОценок пока нет
- Jurnal Subkonjungtiva BleedingДокумент3 страницыJurnal Subkonjungtiva BleedingPuetri 'Poe' SaptlyaОценок пока нет
- Case Report OMEДокумент8 страницCase Report OMEYosephine ninaОценок пока нет
- Referat - Spondilitis TB (RSAL)Документ35 страницReferat - Spondilitis TB (RSAL)Angga Yogi LaksmanaОценок пока нет
- Trauma Mata TajamДокумент46 страницTrauma Mata TajamgagisodihapusberooОценок пока нет
- Infeksi NosokomialДокумент29 страницInfeksi NosokomialAlunaficha Melody KiraniaОценок пока нет
- Etiologi Dan Patogenesis Kondiloma Akuminatum-Kelompok 3Документ16 страницEtiologi Dan Patogenesis Kondiloma Akuminatum-Kelompok 3Nitha SarinaОценок пока нет
- 6665 PDFДокумент4 страницы6665 PDFerindah puspowatiОценок пока нет
- Jurnal Silikosis Dengan Pneumothorax PDFДокумент6 страницJurnal Silikosis Dengan Pneumothorax PDFfalisОценок пока нет
- Case Report on Pulmonary TuberculosisДокумент38 страницCase Report on Pulmonary TuberculosisBunga Listia ParamitaОценок пока нет
- Otitis Media AkutДокумент7 страницOtitis Media AkutghostmanzОценок пока нет
- Kaplan, Sadock, Grebb. 1997. Sinopsis Psikiatri Ilmu Pengetahuan Perilaku Psikiatri Klinis Jilid Satu. Jakarta: Binarupa AksaraДокумент2 страницыKaplan, Sadock, Grebb. 1997. Sinopsis Psikiatri Ilmu Pengetahuan Perilaku Psikiatri Klinis Jilid Satu. Jakarta: Binarupa AksaraLordeОценок пока нет
- Rhinosinusitis: Diagnosis and ManagementДокумент40 страницRhinosinusitis: Diagnosis and ManagementMuthia Khanza AbuBakarОценок пока нет
- Paper MataДокумент18 страницPaper Matairawaty purbaОценок пока нет
- Komplikasi RhinosinusitisДокумент54 страницыKomplikasi RhinosinusitisWilda Kamila SungkarОценок пока нет
- Larynx InfectionsДокумент28 страницLarynx InfectionsMuskan GogiaОценок пока нет
- Large Exotropia Surgery Using Hangback TechniqueДокумент10 страницLarge Exotropia Surgery Using Hangback TechniqueBlack Clover IdОценок пока нет
- Modul Wound Bed Preparation DR Ardianto SucintaДокумент37 страницModul Wound Bed Preparation DR Ardianto SucintaArdianto SucintaОценок пока нет
- Anisometropia PDFДокумент2 страницыAnisometropia PDFAulya Adha DiniОценок пока нет
- PPK Perdoski 2017 Skabies (English)Документ3 страницыPPK Perdoski 2017 Skabies (English)yumizoneОценок пока нет
- PharmFree medical student exchange ItalyДокумент1 страницаPharmFree medical student exchange ItalyTasya BaktaОценок пока нет
- At-A-Glance: Human Papillomavirus InfectionsДокумент26 страницAt-A-Glance: Human Papillomavirus Infectionsketty putriОценок пока нет
- KUALIFIKASI LUKA PADA KESIMPULAN VISUM HIDUPДокумент22 страницыKUALIFIKASI LUKA PADA KESIMPULAN VISUM HIDUPCecep Kurnia SОценок пока нет
- BEDAH UMUM FKUI - Penatalaksanaan ApendisitisДокумент7 страницBEDAH UMUM FKUI - Penatalaksanaan ApendisitisRifda LatifaОценок пока нет
- Keratitis PPT 1 SUB ENGLISHДокумент33 страницыKeratitis PPT 1 SUB ENGLISHarif rhОценок пока нет
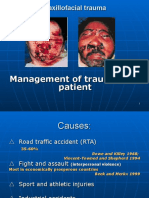
- Primary Management of Maxillofacial TraumaДокумент34 страницыPrimary Management of Maxillofacial TraumafitsumОценок пока нет
- Dead On ArrivalДокумент35 страницDead On ArrivalFitria Diah Suharjo100% (1)
- CombinedДокумент3 страницыCombinedSolape Akin-WilliamsОценок пока нет
- Cutaneous Lupus ErythematosusДокумент15 страницCutaneous Lupus ErythematosusErika KusumawatiОценок пока нет
- Paederus Dermatitis Karthikeyan K, Kumar A - Indian J Dermatol Venereol LeprolДокумент11 страницPaederus Dermatitis Karthikeyan K, Kumar A - Indian J Dermatol Venereol Leprolalmas prawoto100% (1)
- CASE REPORT On ToxoplasmosisДокумент23 страницыCASE REPORT On Toxoplasmosisk.n.e.d.Оценок пока нет
- Healthcare Associated Pneumonia - Dr. Christian A. Johannes, SP - an.KICДокумент30 страницHealthcare Associated Pneumonia - Dr. Christian A. Johannes, SP - an.KICvenyОценок пока нет
- Guideline Konjungtivitis CPG-11 PDFДокумент33 страницыGuideline Konjungtivitis CPG-11 PDFhanumzniiОценок пока нет
- Reflex PupilДокумент21 страницаReflex PupilRaissaОценок пока нет
- Case Report DifteriДокумент20 страницCase Report DifteriKhodimatur RofiahОценок пока нет
- Corne A: Dr. Yulia Fitriani, SPMДокумент47 страницCorne A: Dr. Yulia Fitriani, SPMEdsel QasswaraОценок пока нет
- Referat: Pneumonia in ElderlyДокумент41 страницаReferat: Pneumonia in Elderlyathieqah say-syahidahОценок пока нет
- Olanzapine Vs AripiprazoleДокумент8 страницOlanzapine Vs AripiprazoleDivaviyaОценок пока нет
- K4. Diagnosis Holistik - EngДокумент21 страницаK4. Diagnosis Holistik - EngBevila KorspoilvilОценок пока нет
- Refrst Sindrom KompartementДокумент28 страницRefrst Sindrom Kompartementdesti cahyantiОценок пока нет
- Abses Preaurikula Final 1Документ9 страницAbses Preaurikula Final 1syafiqОценок пока нет
- Hydranencephaly: A Rare Cause of An Enlarging Head Size in An InfantДокумент3 страницыHydranencephaly: A Rare Cause of An Enlarging Head Size in An InfantdyahОценок пока нет
- Derajat Paresis Nervus FasialisДокумент1 страницаDerajat Paresis Nervus FasialisDiah HayustiningsihОценок пока нет
- Continuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress SyndromeДокумент4 страницыContinuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress Syndromelaudya100% (1)
- Tuberculosis 1. Background of The Problem Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With VaricellaДокумент6 страницTuberculosis 1. Background of The Problem Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With VaricellaFkrygeustobat Tikamarimunteupercaya TanyakeunkajalminaОценок пока нет
- Signs and SymptomsДокумент6 страницSigns and SymptomsKajim SharibiОценок пока нет
- Chickenpox: 2008/9 Schools Wikipedia Selection Health and MedicineДокумент5 страницChickenpox: 2008/9 Schools Wikipedia Selection Health and MedicinenvijaykanthОценок пока нет
- Drug Therapy in PregnancyДокумент37 страницDrug Therapy in PregnancyiqiqiqiqiqОценок пока нет
- Infeksi Dalam Kehamilan - EnglishДокумент34 страницыInfeksi Dalam Kehamilan - EnglishFadel Aneuk NanggroeОценок пока нет
- Bladder: Male Urethra and Its SegmentsДокумент33 страницыBladder: Male Urethra and Its SegmentsYohana Elisabeth GultomОценок пока нет
- Strikture UretraДокумент13 страницStrikture UretraFadel Aneuk NanggroeОценок пока нет
- Striktur UretraДокумент2 страницыStriktur UretraFadel Aneuk NanggroeОценок пока нет
- Striktur UretraДокумент12 страницStriktur UretraFadel Aneuk NanggroeОценок пока нет
- Striktur UretraДокумент6 страницStriktur UretraFadel Aneuk NanggroeОценок пока нет
- IMCI-CD POST TEST REVIEWДокумент10 страницIMCI-CD POST TEST REVIEWAngel YN Patricio FlorentinoОценок пока нет
- S-I-R Model Model - NotesДокумент1 страницаS-I-R Model Model - NotesDean WoodОценок пока нет
- Rodriguez, Et Al. 2004. MPC Fluoroquinolones For M.tuberculosisДокумент4 страницыRodriguez, Et Al. 2004. MPC Fluoroquinolones For M.tuberculosisraindrasОценок пока нет
- CertificateДокумент1 страницаCertificatenazmulОценок пока нет
- Key elements of viruses and viral infectionsДокумент44 страницыKey elements of viruses and viral infectionsMay BerОценок пока нет
- DDs of Fever With RashДокумент18 страницDDs of Fever With RashEBОценок пока нет
- Opportunistic Infections: Dr. Baldev S. PrajapatiДокумент69 страницOpportunistic Infections: Dr. Baldev S. PrajapatiZazzZaffaОценок пока нет
- File S1 Survey Questionnaire For Antibiotic Use and Antimicrobial ResistanceДокумент18 страницFile S1 Survey Questionnaire For Antibiotic Use and Antimicrobial ResistancePitua IvaanОценок пока нет
- MeaslesДокумент14 страницMeaslesCHALIE MEQUОценок пока нет
- MCQs in para (With Answers)Документ20 страницMCQs in para (With Answers)janiceli020785% (26)
- Foreword: OIE Terrestrial Manual 2008 IIIДокумент8 страницForeword: OIE Terrestrial Manual 2008 IIIWormInchОценок пока нет
- Nursing responsibilities for ampicillinДокумент3 страницыNursing responsibilities for ampicillinCharlene Serino JavierОценок пока нет
- Head Lice Infestation GuideДокумент17 страницHead Lice Infestation GuideAstuti Clara Simanjuntak100% (1)
- Influenza Teaching Current Update 2023 by Dr.T.V.Rao MDДокумент100 страницInfluenza Teaching Current Update 2023 by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- Welcome To Deped TV Mapeh 8 Class: I Am Aprilyn Grace Ganado ofДокумент42 страницыWelcome To Deped TV Mapeh 8 Class: I Am Aprilyn Grace Ganado ofAprilyn Grace GanadoОценок пока нет
- Ringworm Guide: Symptoms, Types, and TreatmentДокумент5 страницRingworm Guide: Symptoms, Types, and TreatmentAnnisa SyaflianiОценок пока нет
- Primegen laboratoriesPG2 2694 - 2021071918 - 56 - 04 - Primegen Laboratorieslocation1sarscov2covid 19 DetectionДокумент1 страницаPrimegen laboratoriesPG2 2694 - 2021071918 - 56 - 04 - Primegen Laboratorieslocation1sarscov2covid 19 DetectionKeights IndiaОценок пока нет
- Mosquito ControlДокумент284 страницыMosquito Controlrijade100% (1)
- Proctitis Is Inflammation of The Lining of The RectumДокумент2 страницыProctitis Is Inflammation of The Lining of The RectumEllysabet DianОценок пока нет
- Dazomet DrugДокумент2 страницыDazomet Drugashley11Оценок пока нет
- MICHIGAN 2009 IMMUNIZATION WAIVER FORM SS Imm Waiver 2009Документ1 страницаMICHIGAN 2009 IMMUNIZATION WAIVER FORM SS Imm Waiver 2009DonnaОценок пока нет
- Daftar PustakaДокумент3 страницыDaftar PustakaAnonymous P5sbWHRОценок пока нет
- PyodermaДокумент19 страницPyodermaNewton LongjamОценок пока нет
- SG Clean Checklist-Cruise TerminalДокумент8 страницSG Clean Checklist-Cruise TerminallukmannyeoОценок пока нет
- Elc093 November 2021 Final Test - Question PaperДокумент13 страницElc093 November 2021 Final Test - Question PaperNik Ahmad Amirul AimanОценок пока нет
- Typhoid fever: A deadly bacterial infectionДокумент8 страницTyphoid fever: A deadly bacterial infectionMARIANTO PUTRA SUHARDIОценок пока нет
- Dengue: What Is Dengue Fever? What Is Dengue Hemorrhagic Fever?Документ9 страницDengue: What Is Dengue Fever? What Is Dengue Hemorrhagic Fever?Abdul Shakur FaisalОценок пока нет
- (MT 6322 - MYCO VIRO LAB) Unit 7 Laboratory Diagnosis For Negative-Sense (-) ssRNA VirusesДокумент15 страниц(MT 6322 - MYCO VIRO LAB) Unit 7 Laboratory Diagnosis For Negative-Sense (-) ssRNA VirusesAbbas MaghazehiОценок пока нет