Вам также может понравиться
- The Correlation Between Obesity and Prediabetes Among The Student of Lampung University 2013Документ7 страницThe Correlation Between Obesity and Prediabetes Among The Student of Lampung University 2013Uli Kartika SihalohoОценок пока нет
- Sihaloho Uli Kartika, Zuraida Reni, Susianti, Indriani Yaktiworo Medical Faculty of Lampung UniversityДокумент10 страницSihaloho Uli Kartika, Zuraida Reni, Susianti, Indriani Yaktiworo Medical Faculty of Lampung UniversityUli Kartika SihalohoОценок пока нет
- Follow UpДокумент31 страницаFollow UpUli Kartika SihalohoОценок пока нет
- Peningkatan Pengetahuan Anak-Anak Tentang Phbs Dan Penyakit Menular Melalui Teknik Kie Berupa Permainan ElektronikДокумент9 страницPeningkatan Pengetahuan Anak-Anak Tentang Phbs Dan Penyakit Menular Melalui Teknik Kie Berupa Permainan ElektronikUli Kartika SihalohoОценок пока нет
- Nutrional Status of School Age Children PDFДокумент8 страницNutrional Status of School Age Children PDFUli Kartika SihalohoОценок пока нет
- Nutrition Knowledge, Attitude, and Behavior of PDFДокумент13 страницNutrition Knowledge, Attitude, and Behavior of PDFUli Kartika SihalohoОценок пока нет
- Nutritional Status of Under-Five Children Living inДокумент7 страницNutritional Status of Under-Five Children Living inUli Kartika SihalohoОценок пока нет
- Mother and Child Nutrition in The Tropics and SubtДокумент16 страницMother and Child Nutrition in The Tropics and SubtUli Kartika SihalohoОценок пока нет
- Impact of A Nutrition Education Programme On The Nutritional Status of ChildrenДокумент323 страницыImpact of A Nutrition Education Programme On The Nutritional Status of ChildrenUli Kartika SihalohoОценок пока нет
- The Effect of A Nutrition Education ModuleДокумент58 страницThe Effect of A Nutrition Education ModuleUli Kartika Sihaloho100% (1)
- Nutritional Status of Under-Five Children Living inДокумент7 страницNutritional Status of Under-Five Children Living inUli Kartika SihalohoОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- CapstoneДокумент23 страницыCapstoneA - CAYAGA, Kirby, C 12 - HermonОценок пока нет
- Mahindra & MahindraДокумент13 страницMahindra & MahindraAbhishek DharmadhikariОценок пока нет
- Eng DS Epp-2314 1410Документ2 страницыEng DS Epp-2314 1410MarkusAldoMaquОценок пока нет
- Lec 4 - 4th WeekДокумент40 страницLec 4 - 4th Weekrajpoot aliОценок пока нет
- MTH100Документ3 страницыMTH100Syed Abdul Mussaver ShahОценок пока нет
- Updated G10 Class Routine Effective From 12 January 2023Документ1 страницаUpdated G10 Class Routine Effective From 12 January 2023NiloyОценок пока нет
- Table Equivalent Schedule 40 Steel PipeДокумент1 страницаTable Equivalent Schedule 40 Steel PipeorisОценок пока нет
- Board Replacement CasesДокумент41 страницаBoard Replacement CasesNadeeshОценок пока нет
- 1762 Ob8 PDFДокумент16 страниц1762 Ob8 PDFRodríguez EdwardОценок пока нет
- Indor Lighting DesignДокумент33 страницыIndor Lighting DesignRajesh MalikОценок пока нет
- Straight LineДокумент15 страницStraight LineAyanОценок пока нет
- Mean Variance Portfolio TheoryДокумент85 страницMean Variance Portfolio TheoryEbenezerОценок пока нет
- Impact of Retrofitting Existing Combined Heat and Power Plant With Polygeneration of Biomethane PDFДокумент16 страницImpact of Retrofitting Existing Combined Heat and Power Plant With Polygeneration of Biomethane PDFAwais Salman0% (1)
- Health Promotion Throughout The Life Span 7th Edition Edelman Test BankДокумент35 страницHealth Promotion Throughout The Life Span 7th Edition Edelman Test Bankcourtneyharrisbpfyrkateq100% (17)
- Dual Shield 7100 Ultra: Typical Tensile PropertiesДокумент3 страницыDual Shield 7100 Ultra: Typical Tensile PropertiesDino Paul Castro HidalgoОценок пока нет
- Proefschrift T. Steenstra - tcm24-268767Документ181 страницаProefschrift T. Steenstra - tcm24-268767SLAMET PAMBUDIОценок пока нет
- Esteem 1999 2000 1.3L 1.6LДокумент45 страницEsteem 1999 2000 1.3L 1.6LArnold Hernández CarvajalОценок пока нет
- Liver: Anatomy & FunctionsДокумент18 страницLiver: Anatomy & FunctionsDR NARENDRAОценок пока нет
- Prestige Institute of Management & Research: Guided By:-Submitted By: - Prof. Arpit Loya Sumeet RattanДокумент21 страницаPrestige Institute of Management & Research: Guided By:-Submitted By: - Prof. Arpit Loya Sumeet RattanSumeet700005Оценок пока нет
- Highway-And-Railroad-Engineering SummaryДокумент15 страницHighway-And-Railroad-Engineering SummaryRodin James GabrilloОценок пока нет
- Immigrant Italian Stone CarversДокумент56 страницImmigrant Italian Stone Carversglis7100% (2)
- User'S Guide: Tm4C Series Tm4C129E Crypto Connected Launchpad Evaluation KitДокумент36 страницUser'S Guide: Tm4C Series Tm4C129E Crypto Connected Launchpad Evaluation KitLương Văn HưởngОценок пока нет
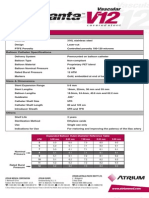
- Advanta V12 Data SheetДокумент2 страницыAdvanta V12 Data SheetJuliana MiyagiОценок пока нет
- Tugas Dikumpulkan Pada Hari Sabtu, 11 April 2020. Apabila Email Bermasalah Dapat Mengirimkan Via WA PribadiДокумент4 страницыTugas Dikumpulkan Pada Hari Sabtu, 11 April 2020. Apabila Email Bermasalah Dapat Mengirimkan Via WA PribadiFebry SugiantaraОценок пока нет
- Someone Who Believes in YouДокумент1 страницаSomeone Who Believes in YouMANOLO C. LUCENECIOОценок пока нет
- 12.5 Collision Theory - ChemistryДокумент15 страниц12.5 Collision Theory - ChemistryAri CleciusОценок пока нет
- Catalogo GatesДокумент255 страницCatalogo GatesBenjamin HedoneweОценок пока нет
- Module 1 Notes The White Bird Reading The Image Painting Analysis PDFДокумент4 страницыModule 1 Notes The White Bird Reading The Image Painting Analysis PDFMelbely Rose Apigo BaduaОценок пока нет
- A Year On A FarmДокумент368 страницA Year On A FarmvehapkolaОценок пока нет
- Significance of GodboleДокумент5 страницSignificance of GodbolehickeyvОценок пока нет