Вам также может понравиться
- The Decline of The Impetigo Epidemic Caused by The Epidemic European Fusidic Acid-Resistant Impetigo Clone: An 11.5-Year Population-Based Incidence Study From A Community in Western NorwayДокумент6 страницThe Decline of The Impetigo Epidemic Caused by The Epidemic European Fusidic Acid-Resistant Impetigo Clone: An 11.5-Year Population-Based Incidence Study From A Community in Western NorwaypataraauliaОценок пока нет
- Koningstein M 12Документ14 страницKoningstein M 12pataraauliaОценок пока нет
- CD 003261Документ165 страницCD 003261pataraauliaОценок пока нет
- Set up PPTP VPN on Windows 8Документ5 страницSet up PPTP VPN on Windows 8pataraauliaОценок пока нет
- J. Antimicrob. Chemother.-2011-Rørtveit-1360-4Документ5 страницJ. Antimicrob. Chemother.-2011-Rørtveit-1360-4pataraauliaОценок пока нет
- Pereira-2014-Anais Brasileiros de DermatologiaДокумент7 страницPereira-2014-Anais Brasileiros de DermatologiapataraauliaОценок пока нет
- Koningstein M 12Документ14 страницKoningstein M 12pataraauliaОценок пока нет
- Non-Hodgkin's Lymphoma of The Stomach: Treatment Outcomes For 57 Patients Over A 20-Year PeriodДокумент5 страницNon-Hodgkin's Lymphoma of The Stomach: Treatment Outcomes For 57 Patients Over A 20-Year PeriodpataraauliaОценок пока нет
- PneumoniaДокумент8 страницPneumoniaPratiwi RukmanaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Republic Act 8504: Philippine AIDS Prevention and Control Act of 1998Документ17 страницRepublic Act 8504: Philippine AIDS Prevention and Control Act of 1998Janah PatriaОценок пока нет
- Tuberculosis: WHO Global Tuberculosis Report 2014Документ2 страницыTuberculosis: WHO Global Tuberculosis Report 2014blueicelandОценок пока нет
- Ayurveda Articles PDFДокумент704 страницыAyurveda Articles PDFAnonymous TWzli5100% (2)
- SEM 2 ChecklistДокумент2 страницыSEM 2 ChecklistYoussef MansourОценок пока нет
- Grand Revalida Study Guide PDFДокумент4 страницыGrand Revalida Study Guide PDFJuanitoCabatañaLimIII100% (1)
- WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues PDFДокумент423 страницыWHO Classification of Tumours of Haematopoietic and Lymphoid Tissues PDFAlejandra Arely López NegreteОценок пока нет
- Menopause Causes Evaluation QuizДокумент27 страницMenopause Causes Evaluation QuizXaa YaaОценок пока нет
- PROTOCOL FOR INDUCING HYPOTHERMIA POST CARDIAC ARRESTДокумент2 страницыPROTOCOL FOR INDUCING HYPOTHERMIA POST CARDIAC ARRESTAnusha VergheseОценок пока нет
- Disease and Immunity - IGCSE NotesДокумент20 страницDisease and Immunity - IGCSE Notesjanani sellapandianОценок пока нет
- FOGSI GCPR On Screening and Vaccination For Prevention of Carcinoma CervixДокумент88 страницFOGSI GCPR On Screening and Vaccination For Prevention of Carcinoma CervixKavitha NarayanaswamyОценок пока нет
- Acute Glomerulonephritis PathophysiologyДокумент4 страницыAcute Glomerulonephritis PathophysiologyJanica Marinas100% (3)
- ClinicalStagesofHIVBiolixir Published2011Документ4 страницыClinicalStagesofHIVBiolixir Published2011Lyzia AushaОценок пока нет
- Evaluation and Management of Common Cardiac ConditionsДокумент104 страницыEvaluation and Management of Common Cardiac ConditionsRatnam hospital100% (1)
- First Prenatal VisitДокумент29 страницFirst Prenatal VisitLucas Phi100% (1)
- Book Let Shama Sharma Research EditДокумент18 страницBook Let Shama Sharma Research Editsai projectОценок пока нет
- Reference For Assignment 2Документ2 страницыReference For Assignment 2chrisОценок пока нет
- Ramacula Potts T11-L1 v4.5Документ10 страницRamacula Potts T11-L1 v4.5Justitia Et PrudentiaОценок пока нет
- Relationship between knowledge level and motivation towards dietary compliance in type 2 diabetes patients: A literature reviewДокумент15 страницRelationship between knowledge level and motivation towards dietary compliance in type 2 diabetes patients: A literature reviewSugiantoОценок пока нет
- History Taking SkillsДокумент39 страницHistory Taking Skillschifunndo charlesОценок пока нет
- PowerpointДокумент29 страницPowerpointpisces200910Оценок пока нет
- Pediatric PallorДокумент2 страницыPediatric PallorSHADHANA SIVAKUMARОценок пока нет
- Ulcer Genitalis EllenoДокумент2 страницыUlcer Genitalis EllenoGabriela Sabatini GunawanОценок пока нет
- Vitamin B12 Treatment Guideline: What Are The Signs of B12 Deficiency?Документ5 страницVitamin B12 Treatment Guideline: What Are The Signs of B12 Deficiency?Yathrika YathrikaОценок пока нет
- Hands On CPRДокумент12 страницHands On CPRMarites PangilinanОценок пока нет
- Hiv V/S Aids: Other Differences Between HIV and AIDS Are Mentioned Below: HIV Is A Virus ThatДокумент1 страницаHiv V/S Aids: Other Differences Between HIV and AIDS Are Mentioned Below: HIV Is A Virus ThatTanya Gupta Srivastava100% (1)
- PhenylketonuriaДокумент7 страницPhenylketonuriaReham QueОценок пока нет
- Characteristics of RTA - UpToDateДокумент2 страницыCharacteristics of RTA - UpToDateKrik AndreiОценок пока нет
- 1436 Cha Editorial Jo Jun 13Документ2 страницы1436 Cha Editorial Jo Jun 13kj0203Оценок пока нет
- Helminth 5Документ5 страницHelminth 5fiena92100% (2)
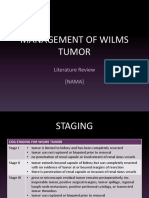
- Management of Wilms Tumor: Literature Review (NAMA)Документ15 страницManagement of Wilms Tumor: Literature Review (NAMA)DeaNataliaОценок пока нет