Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Conflict Management ReportДокумент7 страницConflict Management ReportAnn Michelle Tarrobago100% (1)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Anti-Drug Campaign SpeechДокумент2 страницыAnti-Drug Campaign SpeechGracel Gonzaga Eviota91% (11)
- Schema Focused TherapyДокумент34 страницыSchema Focused TherapyKen Murray100% (6)
- Morality and Ethics - BasicsДокумент23 страницыMorality and Ethics - BasicsAnn Michelle Tarrobago50% (2)
- Sorry Wrong Number by Lucille FletcherДокумент25 страницSorry Wrong Number by Lucille FletcherAnn Michelle Tarrobago100% (6)
- Emergency NursingДокумент19 страницEmergency Nursingshenric16Оценок пока нет
- Introduction To HospitalsДокумент15 страницIntroduction To Hospitalskapgarg50% (2)
- Orthopedic NursingДокумент202 страницыOrthopedic NursingRigo76801100% (3)
- NCLEX Test CVA, Neuro 24Документ19 страницNCLEX Test CVA, Neuro 24Ann Michelle TarrobagoОценок пока нет
- Motivation TheoriesДокумент18 страницMotivation TheoriesMM Ayehsa Allian Schück100% (1)
- DECS Form 178ORIGINALДокумент1 страницаDECS Form 178ORIGINALJhon FurioОценок пока нет
- Role of Clinician in AssessmentДокумент9 страницRole of Clinician in AssessmentTamara Platenkamp100% (1)
- PNI Psychosocial Factors that Impact Immune SystemДокумент23 страницыPNI Psychosocial Factors that Impact Immune SystemAnn Michelle TarrobagoОценок пока нет
- CANCER NSG QuestionsДокумент43 страницыCANCER NSG QuestionsAnn Michelle Tarrobago83% (6)
- Nutrition in The Critically Ill PatientДокумент13 страницNutrition in The Critically Ill PatientnainazahraОценок пока нет
- Maternal and Child Nursing QuestionsДокумент87 страницMaternal and Child Nursing QuestionsAnn Michelle Tarrobago50% (2)
- Pathophysiology (Risk Factors & Symptoms)Документ20 страницPathophysiology (Risk Factors & Symptoms)Ann Michelle TarrobagoОценок пока нет
- ExpoДокумент5 страницExpoAnn Michelle TarrobagoОценок пока нет
- Planning ProcessДокумент10 страницPlanning ProcessAnn Michelle TarrobagoОценок пока нет
- PediatricsДокумент21 страницаPediatricsAnn Michelle TarrobagoОценок пока нет
- Pathophysiology (Risk Factors & Symptoms)Документ20 страницPathophysiology (Risk Factors & Symptoms)Ann Michelle TarrobagoОценок пока нет
- Assessing male infertility and significance of sperm motilityДокумент94 страницыAssessing male infertility and significance of sperm motilityAnn Michelle Tarrobago100% (1)
- Introduction To OrthopaedicsДокумент53 страницыIntroduction To OrthopaedicsAnn Michelle TarrobagoОценок пока нет
- Elements of PoetryДокумент14 страницElements of PoetryAnn Michelle TarrobagoОценок пока нет
- Orthopedic Lecture 06Документ131 страницаOrthopedic Lecture 06Ann Michelle TarrobagoОценок пока нет
- Neuro PlasticityДокумент20 страницNeuro PlasticityAnn Michelle TarrobagoОценок пока нет
- Well-balanced diet and routine tests orderedДокумент8 страницWell-balanced diet and routine tests orderedAnn Michelle TarrobagoОценок пока нет
- I Can Teach and Guide But Not Control Your LifeДокумент1 страницаI Can Teach and Guide But Not Control Your LifeAnn Michelle TarrobagoОценок пока нет
- Leadership StyleДокумент3 страницыLeadership StyleAnn Michelle TarrobagoОценок пока нет
- Gastroenteritis Bronchopneumonia Ear InfectionДокумент34 страницыGastroenteritis Bronchopneumonia Ear InfectionAnn Michelle TarrobagoОценок пока нет
- Goldsman ScoreДокумент1 страницаGoldsman ScoreAnn Michelle TarrobagoОценок пока нет
- NCLEX Review About Immune System Disorders 24Документ12 страницNCLEX Review About Immune System Disorders 24Ann Michelle Tarrobago67% (3)
- NarrativeДокумент1 страницаNarrativeAnn Michelle TarrobagoОценок пока нет
- 2015 Calendar Mini MonthДокумент12 страниц2015 Calendar Mini MonthCherilyn SaagundoОценок пока нет
- June 2015 CalendarДокумент1 страницаJune 2015 CalendarAnn Michelle TarrobagoОценок пока нет
- Indian Calendar With HolidaysДокумент12 страницIndian Calendar With HolidayssmiledepakОценок пока нет
- Definition of DXДокумент2 страницыDefinition of DXAnn Michelle TarrobagoОценок пока нет
- Ethical Issues at The End of LifeДокумент24 страницыEthical Issues at The End of Lifeorderstuff36160100% (1)
- Treatment of Child Victims of Abuse and NeglectДокумент18 страницTreatment of Child Victims of Abuse and NeglectSri Harsha KothapalliОценок пока нет
- Thalassemia: BY: Deddy Ramadhan G2A016098Документ11 страницThalassemia: BY: Deddy Ramadhan G2A016098deddy ramadhanОценок пока нет
- NSK 2013 A00-000-001 enДокумент26 страницNSK 2013 A00-000-001 enThato Merapelo PuleОценок пока нет
- Parkland Formula For Burns Calculated DecisionsДокумент2 страницыParkland Formula For Burns Calculated DecisionsJulia Ines ObregonОценок пока нет
- Medicinal Plants of Sheringal Valley, Dir Upper, KPK, Pakistan PDFДокумент3 страницыMedicinal Plants of Sheringal Valley, Dir Upper, KPK, Pakistan PDFFaiz Ul HaqОценок пока нет
- Catalogue: ProductДокумент24 страницыCatalogue: ProductRavi KrishnanОценок пока нет
- AminoglycosidesДокумент6 страницAminoglycosidesLlosa JuneОценок пока нет
- S - "Sakit Ahong Tinahian" As Verbalized byДокумент6 страницS - "Sakit Ahong Tinahian" As Verbalized bylandilinoОценок пока нет
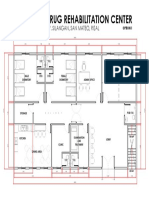
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalДокумент1 страницаProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonОценок пока нет
- Fracture of Radius, Ulna, and HumerusДокумент20 страницFracture of Radius, Ulna, and HumerusAmanda Nur Shinta PertiwiОценок пока нет
- Essential medicines certificateДокумент2 страницыEssential medicines certificateAnji KaringuОценок пока нет
- Cognitive Behavioral Model of Clinical Perfectionism Shafran Cooper Fairburn 2002 En-UsДокумент1 страницаCognitive Behavioral Model of Clinical Perfectionism Shafran Cooper Fairburn 2002 En-UsPavlov PicassoОценок пока нет
- Sensory Deprivation and Loss-4Документ32 страницыSensory Deprivation and Loss-4Scott Daniel Phillips100% (1)
- Joella Pregnancy Support GroupДокумент2 страницыJoella Pregnancy Support GroupElle ctrica100% (2)
- Applying Client-Centred Guidelines to Pediatric OTДокумент7 страницApplying Client-Centred Guidelines to Pediatric OTRaphael AguiarОценок пока нет
- Omeprazole, Potassium Chloride, Citicoline, GlimepirideДокумент5 страницOmeprazole, Potassium Chloride, Citicoline, GlimepirideJenivic Empig PuedanОценок пока нет
- Indira GandhiДокумент8 страницIndira GandhiDanisОценок пока нет
- Pharmacology of Interferons: Mechanisms, Indications, and Treatment of Hepatitis CДокумент30 страницPharmacology of Interferons: Mechanisms, Indications, and Treatment of Hepatitis CRam NareshОценок пока нет
- Sustained Release Dosage FormsДокумент9 страницSustained Release Dosage FormsJasdeep KaurОценок пока нет
- The Differences Between Coaching Mentoring Therapy and Counselling PDFДокумент5 страницThe Differences Between Coaching Mentoring Therapy and Counselling PDFghinaОценок пока нет
- COPD, Asthma, and Lung Disease Nursing Assessment QuestionsДокумент8 страницCOPD, Asthma, and Lung Disease Nursing Assessment QuestionsMichael Boado100% (3)
- 3 ConstipationДокумент18 страниц3 Constipationكسلان اكتب اسميОценок пока нет