IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 1 Ver. IV (Jan. 2015), PP 06-10
www.iosrjournals.org
Increased Incidence of Intracerebral Haemorrhage in winter in
India - a Prospective Study
Dr. Debojyoti Bhattacharjee1, Dr.Kaushik Manna2, Dr. Rajat Kar3, Dr.Kheya
Mukherjee4, Dr.Priyanka Rana5 , Dr. Goutam Chakraborti6 ,
Dr.Swayang Prakash Chowdhury 7
1
Assistant Professor, Department Of Biochemistry,Calcutta National Medical College, Kolkata, West
Bengal, India.
2
Senior Resident, Department Of Cardiology,Calcutta National Medical College, Kolkata, West Bengal,
India.
3
Post graduate student, Department of General Medicine,Calcutta National Medical College, Kolkata,
West Bengal, India.
4
Assistant professor, Department of Microbiology, Nilratan Sircar Medical College, Kolkata, West
Bengal, India.
5
Internee, Department of General Medicine, Calcutta National Medical College, Kolkata, West Bengal, India.
6
Associate Professor, Department Of Biochemistry,Murshidabad Medical College, West Bengal, India.
7
Professor, Endocrinology Unit, Department of General Medicine , Calcutta National Medical College,
Kolkata, West Bengal,India.
I.
Introduction
Cerebrovascular diseases or stroke broadly can be classified into ischemic (85%) and haemorrhagic
(15%) types. The incidence of cerebrovascular diseases increases with age and the number of strokes is
projected to increase as the elderly population grows, with a doubling in stroke deaths [1].
Stroke is the third largest cause of mortality in India after heart attack and cancer [2]. Reliable
morbidity and mortality estimates for stroke in India are limited due to incomplete death certification,
classification, and uncertainty of aetiology in cases of sudden death or multiple co morbidities [3]. The crude
prevalence rates have shown significant regional variation.Age adjusted prevalence rate for stroke is estimated
to lie between 84-262/100,000 in rural and between 334-424/100,000 in urban areas [4]. Several studies from
different countries and climatic zones have demonstrated a seasonal variation in morbidity and cerebrovascular
disease (CVA), but the findings had many discrepancies making the conclusion unclear [5]. The inconsistency
occurred due to small sample size and most of the studies did not analyze the subtypes of strokes. A winter
excess of ischaemic stroke in hospital-based studies is often assumed to be due to seasonal variation in stroke
and several pathophysiological explanations have been proposed in this favour. Lower temperatures in winter
are associated with more mortality than in the summer mostly due to cardiovascular and cerebrovascular events
related to blood pressure (BP) fluctuations in the elderly [6, 7].
In this background our study has been carried out to estimate seasonal variation of stroke and asses the
role of various influencing modifiable factors like BP variation in a tropical region in influencing incidence of
individual stroke types.
II.
Methods
A prospective study was conducted upon 1440 cases of CVA admitted at Calcutta National Medical
College, Kolkata at Calcutta National Medical College and Kolkata between January 2013 and December 2013.
Season was divided as winter (December-February), summer (March-May), monsoon (June-August) and
autumn (September-November). The time of onset of stroke was defined as the time when neurological
symptoms first appeared. The subjects were categorized in to two major groups like ischemic and intracerebral
hemorrhagic stroke based on non contrast brain CT scan and clinical features. Complete clinical history was
noted with special attention to age, season, duration of complaints, family history and personal history like
presence of hypertension, diabetes mellitus, tobacco smoking. Routine blood test including lipid profile was
performed upon all the subjects.
Statistical analysis was done using Statistical Package for Social Science (SPSS-17).For comparing
multiple groups Analysis of Variance (ANOVA) was applied and for comparing two groups t-test was applied.
The critical level of significance was considered at 0.05 level (p<0.05).
DOI: 10.9790/0853-14140610
www.iosrjournals.org
6 | Page
Increased incidence of Intracerebral Haemorrhage in winter in India - A prospective study
III.
Results
A total of 1437 subjects admitted throughout the year were included of which 60.1% were males and 39.9%
were females. The cases were categorized into 4 major groups based on the number of candidates admitted in each
season (TABLE 1). The cases were age and sex matched as far as possible (TABLE 2, 3).The total number of IS and
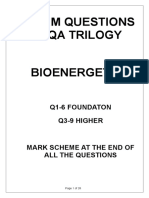
ICH cases in different seasons along with relative percentages were calculated (TABLE 4) and expressed graphically
(Fig1).There was an clear-cut increase in the incidence of ICH cases in winter compared to other seasons .The risk
ratio and 95% confidence interval for the occurrence of ICH stroke in winter compared to summer, monsoon and
autumn was found to be higher (TABLE 5).The difference in systolic and diastolic blood pressure in ICH cases in
winter months compared to rest of the year were found to be significant. However lipid profile values were found to
be almost similar (TABLE 6).
IV.
Discussion
The present study demonstrated a clear seasonal variation in the occurrence of all stroke events in both sexes.
In winters, the overall incidence of stroke was higher among men and women than in rest of the
seasons. This difference was mainly due to ICH, which the most common type of stroke admitted or registered
by far. However, there was also a seasonal difference in the occurrence of ICH [8]. The total number of ICH
cases was highest in winter season compared to other seasons. In fact, the estimates of risk ratios for occurrence
of ICH were higher in winter compared to rest of the seasons. Our results are consistent with findings from other
studies. In a population-based study from Japan, [9] found significant seasonality in the incidence of all strokes,
ICH, and cerebral infarctions. In a community-based stroke register study from Italy, cerebral infarctions were
more frequent during winter and primary ICH during autumn [10]. Some studies have obtained different results
for ICH [11]. Most of the studies in this field have been performed in countries with cold or temperate climates,
but in a study from Israel the average daily incidence of stroke was approximately twice as great on hot days as
on relatively cold days. It suggests that exposure to extreme temperatures, whether cold or hot, may increase the
risk of stroke [12].
Studies in the Finmonica areas of adult Finnish population, noted a significantly higher incidence of IS
and ICH in winter than in summer [13]. In our study the IS case incidence was higher in winter than rest of the
year but much less compared to ICH cases. The biological reasons for the higher occurrence of strokes during
winter are not known, but several possible mechanisms may be suggested. Basic human physiology states that
exposure to cold causes peripheral vasoconstriction and increase in blood pressure [14]. Moreover, total
cholesterol and triglycerides levels tend to be higher in winter than in summer [15]. Most importantly,
considerable seasonal variations, for plasma fibrinogen concentration and viscosity exist in elderly persons
[16,17]. Other factors such as air pollution, exposure to sunlight, incidence of influenza, and diet have been also
suggested to play a role, but variation in temperature has been considered the most likely reason [18].
Review conducted upon the seasonal occurrence of stroke in 2,960 patients at the University of Iowa
from 1978 through 1985 showed that there was a significant increase in the rate of referral for IS during
warmer months. Conversely, the rate of referral for ICH was significantly less during warm weather and rainy
weather [19]. In our study however, statistically significant risk difference for occurrence of ICH was noted
only between winter and summer seasons.
Other findings showed that the incidence of primary intracerebral haemorrhage was increased at low
temperatures, but there was no significant relation between the incidence of ischaemic stroke or subarachnoid
haemorrhage and temperature [20].
In our study except for SBP and DBP significant differences in serum lipid profile between winter and
rest of the season was not observed among ICH cases.SBP and DBP showed significant univariate relationships
with the season more than with temperatures [21]. The suggested aetiology was that cold increases sympathetic
nervous activity, by elevating blood pressure and plasma and urinary catecholamine concentrations [22]. Muscle
sympathetic nerve activity has been reported to have a role in BP regulation in humans. Cutaneous
vasodilatation, loss of water and increased sodium excretion due to sweating cause lower BP in warm
temperatures [23]. Opposite phenomena have been implicated as potential mechanisms for BP rise in cold
conditions.
Vascular wall rigidity also influences BP. Arterial stiffness is related to winter-summer differences in
SBP, but not with DBP. Similarly increased plasma Norepinephrine (NE), plasma renin activity (PRA), and
plasma aldosterone (PA) are thought to participate in mediating hemodynamic changes from summer to winter
[24].
Ninety-six men and women, age range 65-74 years, recruited from a single group general practice in
Cambridge were found to have both systolic (SBP) and diastolic blood pressure (DBP) were greatest during the
winter across the whole distribution of blood pressure. The increase in winter compared to summer was more
evident in subjects with blood pressures > 160/90 mmHg. Older adults show more seasonal BP variation and
this may explains partly the greater cardiovascular disease mortality of elderly subjects during the winter [25].
DOI: 10.9790/0853-14140610
www.iosrjournals.org
7 | Page
Increased incidence of Intracerebral Haemorrhage in winter in India - A prospective study
Similar cross-sectional survey carried out on a rural Ghanaian population, investigating the effect of ambient
temperature on blood pressure in 574 adults aged between 18 and 65 years showed a significant inverse
relationship between ambient temperature and systolic (SBP) and diastolic blood pressure (DBP). SBP fell by 5
mmHg per 10C rise in ambient temperature [26]. Influence of gender on modifying the relationship between
temperature and BP varid from one study result to another [27,28]. Many studies report a seasonal pattern to
stroke which has a strong relationship with BP [26].
In cold conditions, neurohumoral responses help increase heart function and maintain BP and organ
perfusion. However chronic activation of these responses is detrimental causing imbalance between myocardialstimulating and vasoconstricting hormones and between myocardial relaxing and vasodilating hormones [29].
Evidence shows that BP differs between geographical areas. Colder climates are associated with
higher BP measurements. Similarly residents in regions with greater seasonal temperature differences show
greater BP fluctuations [30].
Study conducted upon a large elderly population with hypertension living in a subtropical East
Mediterranean region showed an 18% seasonal variation in BP [31]. Different racial and ethnic groups react
differently to temperature changes. It suggests that temperature is a contributor to the higher cardiovascular
mortality observed in African-Americans compared to Caucasians [32]. Animal model studies show that strokeprone rats have exaggerated BP responses to cold exposure [27].
The limitation of the study includes consideration of cases admitted only in a tertiary care hospital
whereas a large number of stroke patients are admitted in district and sub divisional hospitals. Potential
confounding sources for rise in BP include lifestyle factors such as diet, diurnal variations but these are highly
unlikely considering the cross-sectional nature of the study. Moreover multicentric study upon a larger
population spanning over several years would have probably been helpful to increase the accuracy to determine
relative risk ratio for ICH occurrence in winter compared to other seasons even further. None the less, stroke is
the third largest cause of mortality in India after heart attack and cancer. Given the increasing incidence of ICH
stroke during winter, encouraging physicians to widen the use of long acting antihypertensive drugs would
contribute significantly to the primary prevention of ICH.
V.
Figures And Tables
Table 1: Age and sex distribution of cases across four seasons
MEAN AGE
(In Years) SD
FEMALE
MALE
TOTAL (Season
wise)
TOTAL(rest
of
theyear;summer-autumn)
WINTER
SUMMER
MONSOON
AUTUMN
62.3512.93
(n= 272)
63.2812.32
(n= 373)
62.8212.63
(n= 645)
63.6311.18 (n=104)
63.0811.26
(n= 99)
63.4410.51
(n= 157)
63.2610.89
(n= 256)
63.0311.59
(n= 98)
61.449.66
(n= 187)
62.2410.63
(n= 285)
62.3310.01 (n= 147)
62.9810.59
(n= 251)
62.83 10.7 (n=792)
n= Number of cases; SD=Standard Deviation
Table 2: Analysis of Variance (ANOVA) for mean age (In years)) standard deviation between
cases in different seasons
* p value significant at < 0.05
Table 3: Chi-square test of Independence for number of CVA cases in each sex in various seasons
* p value significant at < 0.05; n: Number of cases
DOI: 10.9790/0853-14140610
www.iosrjournals.org
8 | Page
Increased incidence of Intracerebral Haemorrhage in winter in India - A prospective study
Table 4: Incidence of ICH and IS stroke cases in different seasons
ICH
IS
Total
WINTER
n, (%)
402(62.33)
243(37.67)
645
SUMMER
n, (%)
138(54.99)
113(45.01)
251
MONSOON
n, (%)
155(60.55)
101(39.45)
256
AUTUMN
n, (%)
180(63.16)
105(36.84)
285
Total n, (%)
Rest of the year
473(59.72)
319(40.28)
792
n: Number of cases; ICH: Intracerebral Haemorrhage; IS:Ischaemic Stroke
Table 5 Relative risks for occurrence of ICH stroke in winter compared to other seasons
ICH
INCIDENCE
Odds Ratio
95% CI
z statistics
p value
SUMMER
1.3546
1.0083-1.82
2.015
0.043
WINTER versus
MONSSON
AUTUMN
1.078
0.965
0.801 1.45
0.72 1.29
0.496
0.242
0.62
0.81
Rest of the year
1.1157
0.9 1.38
1.006
0.315
* p value significant at < 0.05; ICH: Intracerebral Haemorrhage; CI: Confidence Interval
Table 6: Comparison of blood pressure levels and serum lipid profile between ICH cases in winter and
rest of the year
(Mean SD)
Systolic blood pressure
Diastolic blood pressure
Serum Cholesterol
Serum Triglyceride
Serum LDL-C
Serum HDL-C
ICH (Winter)
1646 mm of Hg
100 4 mm of Hg
20161 mg%
18060 mg%
13930 mg%
3510 mg%
ICH (Rest of the year)
15410
94 6
20463
17540
13336
3619
p value
< 0.0001
< 0.0001
0.065
0.06
0.071
0.227
* p value significant at < 0.05; SD=Standard Deviation; ICH: Intracerebral Haemorrhage
LDL-C=Low Density Lipoprotein Cholesterol; HDL-C= Density Lipoprotein Cholesterol; Hg=Mercury
Fig 1 Line chart depicting incidence of ICH and IS cases in different seasons
ICH: Intracerebral Haemorrhage; IS:Ischaemic Stroke; n= Number of cases
VI.
Conclusion
The results indicate the need for prospective multicenter studies with serial assessment of modifiable
risk factors like BP, to assess the impact of these factors on prevalence and pathogenesis of ICH.
Bliography
[1].
[2].
[3].
[4].
[5].
[6].
Smith WS, English JD, Johnston SC, Cerebrovascular Diseases,in Longo DL, Fauci AS, Kasper DL et al (Ed.), Harrisons
Principles of Internal Medicine, 18 (New York: Mc Graw Hill,2012) 3271-3272.
Pandian JD , Stroke in India, Annuals of Indian Academy of Neurology, 11,2008, 2-3.
Pandian JD, Srikanth V, Read SJ, Thrift AG, Poverty and stroke in India, Stoke AHA J, 38,2007, 3063-3069.
Banarjee TK, Das SK, Epidemiology of stroke in India, Neurology Asia ,11, 2006, 1-4.
Douglas AS, Allan TM, Rawles JM, Composition of seasonality of Disease, Scot Med, 36,1991,76-82.
Stewart S, McIntyre K, Capewell S, McMurray JJ, Heart failure in a cold climate, Seasonal variation in heart failure-related
morbidity and mortality, J Am Coll Cardiol 39,2002,760-766.
DOI: 10.9790/0853-14140610
www.iosrjournals.org
9 | Page
Increased incidence of Intracerebral Haemorrhage in winter in India - A prospective study
[7].
[8].
[9].
[10].
[11].
[12].
[13].
[14].
[15].
[16].
[17].
[18].
[19].
[20].
[21].
[22].
[23].
[24].
[25].
[26].
[27].
[28].
[29].
[30].
[31].
[32].
Feigin VL, Anderson CS, Anderson NE, Broad JB, Pledger MJ, Bonita R, Is there a temporal pattern in the occurrence of
subarachnoid hemorrhage in the southern hemisphere?Pooled data from 3 large, population- based incidence studies in Australasia,
1981 to 1997, Stroke 32,2001, 613-619.
Tsementzis SA, Kennet RP, Hitchock ER, Gill JS, BeeversD,Seasonal variation of cerebrovascular disease, Acta Neurochir
(Wien).111,1991,80-83.
Shinkawa A, Ueda K, Hasuo Y, Kiyohara Y, Fujishima M, Seasonal variation in stroke incidence in Hisayama,
Japan, Stroke.21,1990,1262-1267.
Ricci S, Grazia Celani M, Vitali R, La Rosa F, Righetti E, Duca E, Diurnal and seasonal variations in the occurrence of stroke: a
community-based Study, Neuroepidemiology11,1992,59-64.
Sobel E, Zhang ZX, Alter M, Lai SM, Davanipour Z, Friday G, McCoy R, Isack T,Levitt L, Stroke in the Lehigh Valley: seasonal
variation in incidence Rates, Stroke 18,1987,38-42.
Berginer VM, Goldsmith J, Batz U, Vardi H, Shapiro Y , Clustering of strokes in association with meteorologic factors in the
Negev Desert of Israel:1981-1983, Stroke 20,1989,65-69.
Jakovljevic D, Salomaa V, Sivenius J et al, Seasonal variation in the occurrence of stroke in a finnish adult population.
The Finmonica stroke register. Finnish monitoring trends and determinants in cardiovascular disease ,Stroke
27(10),1996,1774-9.
Brennan PJ, Greennerg G, Miall WE, Thompson SG, Seasonal variation in arterial blood pressure, BMJ 285,1982,919-923.
Gordon DJ, Hyde J, Trost DC, Whaley FS, Hannan PJ, Jacobs DR, Ekelund LG, Cyclic seasonal variation in plasma lipid and
lipoprotein levels: the Lipid Research Clinics Coronary Primary Prevention Trial placebo group, J Clin Epidemiol 41,1988,679-689.
Woodhouse PR, Khaw KT, Plummer M, Foley A, Meade TW,Seasonal variations of plasma fibrinogen and factor VII activity in
the elderly: winter infections and death from cardiovascular disease, Lancet 343,1994,435-439.
Wilhelmsen L, Swrdsudd K, Korsan-Bengtsen K, Larsson B, Welin L, Tibblin G, Fibrinogen as a risk factor for stroke and
myocardial infarction, N Engl J Med 311,1984,501-505.
Khaw KT, Temperature and cardiovascular mortality, Lancet 345,1995,337-338.
Biller J, Jones MP,Bruno A, AdamsJr HP, Banwart K, Seasonal Variation of Stroke Does it Exist?, Neuroepidemiology
7,1988,89-98.
Rothwell PM, Slattery J, Warlow CP, Wroe SJ, Is stroke incidence related to season or temperature,
J
Hypertens 11(11),1993,1267-74.
Barnett AG, Sans S, Salomaa V, Kuulasmaa K, Dobson AJ,The effect of temperature on systolic blood pressure,
Blood Press Monit 12,2007, 195-203.
Fu Q, Zhang R, Witkowski S, Arbab-Zadeh A, Prasad A,Okazaki K, Levine BD, Persistent sympathetic activation during chronic
antihypertensive therapy: a potential mechanism for long term morbidity? Hypertension 45,2005, 513-521.
Rosenthal T, Seasonal variations in blood pressure, Am J Geriatr Cardiol ,13,2004, 267-272.
Radke KJ, Izzo JL, Seasonal variation in haemodynamics and blood pressure- regulating hormones(2010). J Hum Hypertens
24,2010, 410-416.
Woodhouse PR, Khaw KT, Plummer M ,Seasonal variation of blood pressure and its relationship to ambient temperature in an
elderly population, J Hypertens 11(11),1993,1267-74.
Kunutsor SK, Kunutsor SK, Powles JW, The effect of ambient temperatur on blood pressure in a rural West African adult
population: a cross-sectional study, Cardiovasc J Afr 21(1),2010, 1720.
Takenaka T, Kojima E, Sueyoshi K, Sato T, Uchida K, Arai J, Hoshi H, Kato N, Takane H, Suzuki H, Seasonal variationsof daily
changes in blood pressure among hypertensive patients with end-stage renal diseases, Clin Exp Hypertens 32,2010,227-233.
Kent ST, Howard G, Crosson WL, Prineas RJ, McClure LA, The association of remotely-sensed outdoor temperature with blood
pressure levels in REGARDS: a cross-sectional study of a large, national cohort of African- American and white participants,
Environ Health 10,2011, 7.
Yamazaki F, Heat stress and human baroreflex function, J UOEH 32,2010, 329-340.
Kimura T, Senda S, Masugata H, Yamagami A, Okuyama H,Kohno T, Hirao T, Fukunaga M, Okada H, Goda F, Seasonal blood
pressure variation and its relationship to environmental temperature in healthy elderly Japanese studied by home measurements,
Clin Exp Hypertens 32,2010, 8-12.
Charach G, Rabinovich PD, Weintraub M, Seasonal changes in blood pressure and frequency of related complications in elderly
Israeli patients with essential hypertension, Gerontology 50,2004, 315-321.
Youn JC, Rim SJ, Park S, Ko YG, Kang SM, Choi D, Ha JW,Jang Y, Chung N, Arterial stiffness is related to augmented seasonal
variation of blood pressure in hypertensive patients , Blood Press 16,2007, 375-380
DOI: 10.9790/0853-14140610
www.iosrjournals.org
10 | Page
Вам также может понравиться
- The Effect of Instructional Methods and Locus of Control On Students' Speaking Ability (An Experimental Study in State Senior High School 01, Cibinong Bogor, West Java)Документ11 страницThe Effect of Instructional Methods and Locus of Control On Students' Speaking Ability (An Experimental Study in State Senior High School 01, Cibinong Bogor, West Java)International Organization of Scientific Research (IOSR)Оценок пока нет
- Comparison of Psychological Variables Within Different Positions of Players of The State Junior Boys Ball Badminton Players of ManipurДокумент4 страницыComparison of Psychological Variables Within Different Positions of Players of The State Junior Boys Ball Badminton Players of ManipurInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Effects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaДокумент10 страницEffects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaInternational Organization of Scientific Research (IOSR)100% (1)
- Study The Changes in Al-Ahwaz Marshal Using Principal Component Analysis and Classification TechniqueДокумент9 страницStudy The Changes in Al-Ahwaz Marshal Using Principal Component Analysis and Classification TechniqueInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Comparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockДокумент2 страницыComparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Child Mortality Among Teenage Mothers in OJU MetropolisДокумент6 страницChild Mortality Among Teenage Mothers in OJU MetropolisInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Project Based Learning Tools Development On Salt Hydrolysis Materials Through Scientific ApproachДокумент5 страницProject Based Learning Tools Development On Salt Hydrolysis Materials Through Scientific ApproachInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Philosophical Analysis of The Theories of Punishment in The Context of Nigerian Educational SystemДокумент6 страницPhilosophical Analysis of The Theories of Punishment in The Context of Nigerian Educational SystemInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Necessary Evils of Private Tuition: A Case StudyДокумент6 страницNecessary Evils of Private Tuition: A Case StudyInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Development of Dacum As Identification Technique On Job Competence Based-Curriculum in High Vocational EducationДокумент5 страницDevelopment of Dacum As Identification Technique On Job Competence Based-Curriculum in High Vocational EducationInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Enhancing Pupils' Knowledge of Mathematical Concepts Through Game and PoemДокумент7 страницEnhancing Pupils' Knowledge of Mathematical Concepts Through Game and PoemInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Microencapsulation For Textile FinishingДокумент4 страницыMicroencapsulation For Textile FinishingInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Students' Perceptions of Grammar Teaching and Learning in English Language Classrooms in LibyaДокумент6 страницStudents' Perceptions of Grammar Teaching and Learning in English Language Classrooms in LibyaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Youth Entrepreneurship: Opportunities and Challenges in IndiaДокумент5 страницYouth Entrepreneurship: Opportunities and Challenges in IndiaInternational Organization of Scientific Research (IOSR)100% (1)
- Need of Non - Technical Content in Engineering EducationДокумент3 страницыNeed of Non - Technical Content in Engineering EducationInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Geohydrological Study of Weathered Basement Aquifers in Oban Massif and Environs Southeastern Nigeria: Using Remote Sensing and Geographic Information System TechniquesДокумент14 страницGeohydrological Study of Weathered Basement Aquifers in Oban Massif and Environs Southeastern Nigeria: Using Remote Sensing and Geographic Information System TechniquesInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Lipoproteins and Lipid Peroxidation in Thyroid DisordersДокумент6 страницLipoproteins and Lipid Peroxidation in Thyroid DisordersInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Comparison of Selected Anthropometric and Physical Fitness Variables Between Offencive and Defencive Players of Kho-KhoДокумент2 страницыComparison of Selected Anthropometric and Physical Fitness Variables Between Offencive and Defencive Players of Kho-KhoInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Auxin Induced Germination and Plantlet Regeneration Via Rhizome Section Culture in Spiranthes Sinensis (Pers.) Ames: A Vulnerable Medicinal Orchid of Kashmir HimalayaДокумент4 страницыAuxin Induced Germination and Plantlet Regeneration Via Rhizome Section Culture in Spiranthes Sinensis (Pers.) Ames: A Vulnerable Medicinal Orchid of Kashmir HimalayaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Comparative Effect of Daily Administration of Allium Sativum and Allium Cepa Extracts On Alloxan Induced Diabetic RatsДокумент6 страницComparative Effect of Daily Administration of Allium Sativum and Allium Cepa Extracts On Alloxan Induced Diabetic RatsInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Advancing Statistical Education Using Technology and Mobile DevicesДокумент9 страницAdvancing Statistical Education Using Technology and Mobile DevicesInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Study of Effect of Rotor Speed, Combing-Roll Speed and Type of Recycled Waste On Rotor Yarn Quality Using Response Surface MethodologyДокумент9 страницStudy of Effect of Rotor Speed, Combing-Roll Speed and Type of Recycled Waste On Rotor Yarn Quality Using Response Surface MethodologyInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Application of Xylanase Produced by Bacillus Megaterium in Saccharification, Juice Clarification and Oil Extraction From Jatropha Seed KernelДокумент8 страницApplication of Xylanase Produced by Bacillus Megaterium in Saccharification, Juice Clarification and Oil Extraction From Jatropha Seed KernelInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Core Components of The Metabolic Syndrome in Nonalcohlic Fatty Liver DiseaseДокумент5 страницCore Components of The Metabolic Syndrome in Nonalcohlic Fatty Liver DiseaseInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Investigation of Wear Loss in Aluminium Silicon Carbide Mica Hybrid Metal Matrix CompositeДокумент5 страницInvestigation of Wear Loss in Aluminium Silicon Carbide Mica Hybrid Metal Matrix CompositeInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Factors Affecting Success of Construction ProjectДокумент10 страницFactors Affecting Success of Construction ProjectInternational Organization of Scientific Research (IOSR)Оценок пока нет
- A Review On Refrigerants, and Effects On Global Warming For Making Green EnvironmentДокумент4 страницыA Review On Refrigerants, and Effects On Global Warming For Making Green EnvironmentInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Research Analysis On Sustainability Opportunities and Challenges of Bio-Fuels Industry in IndiaДокумент7 страницResearch Analysis On Sustainability Opportunities and Challenges of Bio-Fuels Industry in IndiaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Parametric Optimization of Single Cylinder Diesel Engine For Specific Fuel Consumption Using Palm Seed Oil As A BlendДокумент6 страницParametric Optimization of Single Cylinder Diesel Engine For Specific Fuel Consumption Using Palm Seed Oil As A BlendInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Farmakologi Antiagina TTMДокумент83 страницыFarmakologi Antiagina TTMEpha Lumban GaolОценок пока нет
- ReportДокумент10 страницReportSems AlcozbaryОценок пока нет
- February Month Brain DiscussionДокумент63 страницыFebruary Month Brain DiscussionJulyhathul KuraishiОценок пока нет
- Identify The Part of The BrainДокумент2 страницыIdentify The Part of The BrainClement Mar ClimacoОценок пока нет
- Salami Zupcaste PumpeДокумент36 страницSalami Zupcaste PumpeAdmir RamicОценок пока нет
- Blood Supply of BrainДокумент49 страницBlood Supply of BrainDarling Sevenfoldism SynysterОценок пока нет
- Biology: Sexual ReproductionДокумент7 страницBiology: Sexual ReproductionAllan BustamanteОценок пока нет
- Cellular ComponentsДокумент2 страницыCellular ComponentsWangSheng TanОценок пока нет
- Artificial OrgansДокумент184 страницыArtificial OrganshemavathyrajasekaranОценок пока нет
- Exam Questions Aqa Trilogy Bioenergetics: Q1-6 Foundaton Q3-9 HigherДокумент28 страницExam Questions Aqa Trilogy Bioenergetics: Q1-6 Foundaton Q3-9 Higherapi-422428700Оценок пока нет
- Review of Placenta DeliveryДокумент3 страницыReview of Placenta DeliverygitapramodhaОценок пока нет
- g12 Bone Grafts Subs JTG Rev 10 17 10Документ57 страницg12 Bone Grafts Subs JTG Rev 10 17 10Tudor RalucaОценок пока нет
- Introduction to Biomolecules and Cellular ComponentsДокумент18 страницIntroduction to Biomolecules and Cellular ComponentsM Nur M. MahmudОценок пока нет
- Veta 3 - Datasheet - ENG - 20210315Документ2 страницыVeta 3 - Datasheet - ENG - 20210315JuanОценок пока нет
- Levels of Organization Power Point and ActivityДокумент8 страницLevels of Organization Power Point and ActivityJudy RianoОценок пока нет
- Auditory Pathways: Anatomy and Physiology: Handbook of Clinical Neurology March 2015Документ24 страницыAuditory Pathways: Anatomy and Physiology: Handbook of Clinical Neurology March 2015florensiaОценок пока нет
- Apgar ScoreДокумент11 страницApgar Scorefaizura100% (1)
- Paget Disease Causes Excessive Bone Formation and DeformationДокумент14 страницPaget Disease Causes Excessive Bone Formation and DeformationOrson SimonОценок пока нет
- Human Anatomy and Physiology Study Guide 1Документ12 страницHuman Anatomy and Physiology Study Guide 1api-637418753Оценок пока нет
- Nephrology Block Ia. History: A. InformantДокумент4 страницыNephrology Block Ia. History: A. InformantKatherine FabrosОценок пока нет
- Classification and Types of StrokeДокумент11 страницClassification and Types of StrokeJose Enrique OrtizОценок пока нет
- UEP Biochemistry Module 1 IntroductionДокумент24 страницыUEP Biochemistry Module 1 IntroductionCent VinОценок пока нет
- Case StudyДокумент3 страницыCase StudyAnonymous Gof8o3Оценок пока нет
- Aerobic Respiration: Chemiosmosis and Electron Transport ChainДокумент17 страницAerobic Respiration: Chemiosmosis and Electron Transport ChainAihk kenneth BaronaОценок пока нет
- Interoception-201 March-2019Документ38 страницInteroception-201 March-2019api-526165635Оценок пока нет
- Hubungan Kadar Hemoglobin Dan Tercapainya Remisi Pada Anak Penderita Leukemia AkutДокумент7 страницHubungan Kadar Hemoglobin Dan Tercapainya Remisi Pada Anak Penderita Leukemia AkutRezky RahmadayantiОценок пока нет
- Chap 12Документ86 страницChap 12chemptnkОценок пока нет
- LingalaДокумент4 страницыLingalaFabio Ando Filho0% (1)
- Course Outline For 125:355, Physiological Systems For Biomedical EngineersДокумент2 страницыCourse Outline For 125:355, Physiological Systems For Biomedical EngineersbillОценок пока нет
- GyyggДокумент11 страницGyyggYaumil AqsaОценок пока нет