Human Immunology 75 (2014) 11971202
Contents lists available at ScienceDirect
www.ashi-hla.org
journal homepage: www.elsevier.com/locate/humimm
Association of MASP2 polymorphisms and protein levels with rheumatic
fever and rheumatic heart disease
Sandra Jeremias dos Santos Catarino a, Angelica Beate Winter Boldt a,b, Marcia Holsbach Beltrame a,
Renato Mitsunori Nisihara a, Marcelo Derbli Schafranski c, Iara Jose de Messias-Reason a,
a
b
c
Laboratrio de Imunopatologia Molecular, Departamento de Patologia Mdica, Hospital de Clnicas, Universidade Federal do Paran, Curitiba, Brazil
Departamento de Gentica, Universidade Federal do Paran, Curitiba, Brazil
Departamento de Medicina, Universidade Estadual de Ponta Grossa, Paran, Brazil
a r t i c l e
i n f o
Article history:
Received 21 March 2014
Accepted 6 October 2014
Available online 12 October 2014
Keywords:
Rheumatic fever
Rheumatic heart disease
MASP2
Polymorphism
Haplotype-specic genotyping
a b s t r a c t
MASP-2 is a key protein of the lectin pathway of complement system. Several MASP2 polymorphisms
were associated with MASP-2 serum levels or functional activity. Here we investigated a possible association between MASP2 polymorphisms and MASP-2 serum levels with the susceptibility to rheumatic
fever (RF) and rheumatic heart disease (RHD). We haplotyped 11 MASP2 polymorphisms with multiplex
sequence-specic PCR in 145 patients with history of RF from south Brazil (103 with RHD and 42 without
cardiac lesion [RFo]) and 342 healthy controls. MASP-2 levels were determined by ELISA. The low MASP-2
producing p.377A and p.439H variants were negatively associated with RF (P = 0.02, OR = 0.36) and RHD
(P = 0.01, OR = 0.25). In contrast, haplotypes that share the intron 9 exon 12 g.1961795C, p.371D,
p.377V and p.439R polymorphisms increased the susceptibility to RHD (P = 0.02, OR = 4.9). MASP-2 levels
were associated with MASP2 haplotypes and were lower in patients (P < 0.0001), which may reect
protein consumption due to complement activation. MASP2 gene polymorphisms and protein levels seem
to play an important role in the development of RF and establishment of RHD.
2014 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights
reserved.
1. Introduction
Rheumatic fever (RF) and its most severe sequel chronic rheumatic heart disease (RHD) are chronic inammations that follow
oropharynx infection by b-hemolytic Streptococcus group A. The
disease occurs in genetically predisposed children and teenagers
(aged 319 years) affecting the heart, joints, nervous system and
skin [1]. The onset of RF usually occurs two to three weeks following the initial pharyngitis, but in some cases the onset may be
months later [2]. Carditis is the most severe clinical manifestation
of RF, affecting about 3050% of patients 48 weeks after the rst
RF episode [3]. In general, carditis progress to RHD, associated with
chronic inammation and stenosis of valve tissue, leading to permanent heart damage. RHD affects young adults and remains a
Abbreviations: MASP-2, mannan-binding lectin-associated serine protease 2;
MASP2, MASP-2 gene; MBL, mannan-binding lectin; RF, rheumatic fever; RHD,
rheumatic heart disease.
Corresponding author at: Laboratrio de Imunopatologia Molecular, Servio
de Anatomia Patolgica, Hospital de Clnicas, Federal University of Paran (UFPR),
R. General Carneiro, 181, CEP 80060-900 Curitiba, PR, Brazil.
E-mail address: iarareason@hc.ufpr.br (I.J. de Messias-Reason).
major public health problem in Brazil and other developing countries, due to high morbidity and mortality. RF incidence exceeds 50
per 100,000 children in some developing countries [4] and RHD
global prevalence varies between 15 and 20 million cases [5].
About two million cases require repeated hospitalization and one
million may need a heart transplant in 520 years, generating high
costs to the health system [1,5,6]. In Brazil, the estimated rate is
10 million cases of streptococcal pharyngitis each year, resulting
in 30,000 new cases of RF, of which approximately 15,000 progress
to RHD [7].
The complement system serves as the backbone of innate
immunity and supports the adaptive immune system in gaining
momentum to respond. At present, more than 40 components of
complement have been described [8]. The complement system is
activated through the classical, alternative and lectin pathways.
Complement activation leads to recruitment of inammatory
mediators, pathogen destruction and clearance of immune complexes and apoptotic cells [9,10]. The lectin pathway is initiated
by the binding of mannose-binding lectin (MBL) or colins to carbohydrates or acetylated residues on the surface of pathogens,
respectively [11]. MBL and colins are associated with serine
http://dx.doi.org/10.1016/j.humimm.2014.10.003
0198-8859/ 2014 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights reserved.
1198
S.J.d.S. Catarino et al. / Human Immunology 75 (2014) 11971202
proteases named MBL-associated serine proteases 1 and 2
(MASP-1 and MASP-2), which mediate the formation of C3
convertase [11].
MASP-2 and MAp19 (also known as sMAP or small MAP) are
encoded by the MASP2 gene, located on 1p36.23-31. MAp19 is a
truncated protein resulting from alternative splicing and inclusion
of exon 5 in the mature mRNA [12]. MASP-2 and MAp19 share two
domains encoded by the rst four exons (CUB1 C1r/C1s, Uegf and
bone morphogenetic protein-1 and an epidermal growth factor
(EGF)-like domain). Exon 5 encodes the four last amino acids
exclusive of MAp19. Exons 611 encode a second CUB domain
(CUB2) and two contiguous complement control protein modules
(CCP1 and CCP2). Exon 12 encodes the activating peptide and serine protease domain [13]. MASP-2 plays a key role in the activation
of the lectin pathway initiated by colins, colectin 11 or MBL.
MAp19 binds MBL, but its function remains speculative [14].
MASP-2 deciency was rst described in a patient with multiple
infections and autoimmune manifestations, due to an exon 3
mutation causing the exchange of aspartic acid with glycine at
position 120 (p.D120G) [15]. Several other MASP2 polymorphisms,
including g.1945560C>A in the promoter region, p.R99Q and
p.P126L in exon 3, g.7164A>G in intron 4, g.7441G>A in intron 5,
g.1961795C>T in intron 9, p.D371Y and p.V377A in exon 10,
p.R439H and g.24762C>T in exon 12, were found associated with
serum levels or functional activity of MASP-2 [1619]. Some of
them (p.126L, p.377A, p.439H associated with low MASP-2 levels
and p.371D associated with high MASP-2 levels probably due to
linkage disequilibrium with intronic variants) were associated
with susceptibility to diseases: leprosy [19], hepatitis C [20],
malaria [21], bacterial infections after orthotopic liver transplantation [22], Chagas disease [23] and rheumatoid arthritis [24].
These SNPs are distributed in ten main haplotypes comprised of
four variant blocks. The rst block contains the promoter variant at
nucleotide position 1945560 and three amino acid variants at
codons 99, 120 and 126 (ARDP, ARGP, CRDP, CQDP, CRDL); the second block contains the intron 4 and 5 variants (AG, GA, GG), the
third block by the intron 9 and two amino acid variants at codons
371 and 377 (CDA, CDV, TDV), fourth block contains one amino acid
variant at codon 439 and a synonymous variant at nucleotide position 24762 (RC, HC, RT). For practical reasons, the haplotypes were
named according to their phylogenetic relationships. Five haplotypes belong to clade 1 and share g.24762C in exon 12. Among
them, 1A represents the most ancient haplotype, 1B1-h and
1B2-h share g.1961795T in intron 9 and are associated with higher
MASP-2 levels (reason for the h sufx), 1C1-l and 1C2-l share
p.126L and are associated with low MASP-2 levels (reason for the
l sufx). Importantly, 1C2-l also bears the deciency-causing
p.439H variant. Five other haplotypes belong to clade 2 and present g.24762T in exon 12: 2A1, 2A2-l (with p.377A), 2B1-i and
2B2A-i (both associated with intermediate i MASP-2 levels),
and the MASP-2 deciency-causing 2B2B-l haplotype (with the
p.120G variant) [18]. Variants in introns 4 and 5 mainly occur as
two combinations in cis, AG and GA, in the 1A, 1B1-h, 2A1,
2B1-I and 2B2A-I haplotypes, reason for which they are added
between clasps after the haplotype name (e.g. 1A [AG]). These
polymorphisms probably modulate alternative exon 5 splicing,
since GA is associated with higher MASP-2 and lower MAp19 levels, the opposite being true for AG [19].
2. Material and methods
2.1. Subjects and samples
This study was approved by the local ethics committee (CEP/HC
2658.265/2011-11). We investigated a total of 145 patients with a
history of RF with mean age of 39 years (range = 1889 years). All
patients had a history of RF and were diagnosed according to Jones
modied criteria [25]. Among them, 103 (71%) had RHD, conrmed
by transthoracic echocardiogram showing rheumatic involvement
of the mitral valve; 42 patients (29%) did not present RHD but
had history of RF and were designated as rheumatic fever only
(RFo) patients. Clinical characterization of RFo and RHD patients
was described in a previous study [26]. None of the patients presented other inammatory disease, neoplasia, infective endocarditis or other infection at the time of blood collection.
The control group included 286 blood donors and 56 health
workers and other volunteers (without history of rheumatic fever)
from the same geographic region, with a mean age of 41.3 years
(range = 1861 years). Among the blood donors, 65 were from
Hospital de Clnicas of the UFPR, 174 were from Centro de
Hemoterapia e Hematologia do Paran (Hemepar) and 47 from
Biobanco of the Hospital Evanglico, paired with the patients
according to age and ancestry. Differences in sex distribution
between patients and controls and in age distribution between
RHD and RFo patients were corrected with multivariate logistic
regression (Table 1).
2.2. MASP2 genotyping
A total of eleven MASP2 single nucleotide polymorphisms
(SNPs) were investigated. Taking NG007289.1 as reference
sequence, they were: g.4847A>C in the promoter (rs7548659),
g.5557G>A (rs61735600), g.5620A>G (rs72550870) and g.5638C>T
(rs56392418) in exon 3 (causing amino acid substitutions
p.R99Q, p.D120G and p.P126L in the CUB1 domain, respectively),
g.7164A>G (rs2273344) in intron 4, g.7441G>A (rs9430347) in
intron 5, g.21081C>T in intron 9 (rs17409276), g.21370G>T
(rs12711521) and g.21389T>C (rs2273346) in exon 10 (causing
amino acid substitutions p.Y371D and p.V377A in the CCP2
domain, respectively) and g.24599G>A (rs12085877) and
g.24762T>C (rs1782455) in exon 12 (encoding one non synonymous p.R439H and one synonymous variant p.S493=). Minor
intronic alleles (g.7164G, g.7441A and g.21081T) have been formerly
associated with MASP-2 levels higher than 600 ng/ml [18,19],
whereas minor non synonymous alleles encoding p.120G, p.126L,
p.377A and p.439H were associated with MASP-2 levels lower than
200 ng/ml. Among them, homozygotes for p.120G or p.439H are
unable to activate the lectin pathway of complement [16,17]. The
SNPs were identied by a multiplex sequence-specic amplication method (multiplex PCR-SSP), as previously described [18,19].
2.3. MASP-2 assay
MASP-2 concentrations were measured in the sera of 145
patients (42 RFo and 103 RHD) and 196 controls using enzymelinked immunosorbent assay (HK326, Hycult Biotechnology, Uden,
The Netherlands). Both groups were homogeneous regarding
MASP2 genotype distribution. Minimum concentration which can
be measured is 1.6 ng/ml. Color intensity was evaluated at
450 nm in an ELISA reader.
2.4. Statistics
Genotype, allele and haplotype frequencies were obtained by
direct counting. SNPs distributed from the promoter to exon 12
were phased with the SSP primers. In most cases, the phase
between distantly situated SNPs could be deduced due to strong
linkage disequilibrium between the variants [18]. Hardy
Weinberg equilibrium and homogeneity between genotype
distributions were tested using ARLEQUIN software package
version 3.5.1.3 [27]. MASP-2 levels were tested for normality
1199
S.J.d.S. Catarino et al. / Human Immunology 75 (2014) 11971202
Table 1
Demographic characteristics of RF and RHD patients.
n
Male (%)
Female (%)
Euro-Brazilians (%)
Afro-Brazilians (%)
Mean age SD
Mean age female SD
Mean age male SD
n
Male (%)
Female (%)
Euro-Brazilians (%)
Afro-Brazilians (%)
Mean age SD
Mean age female SD
Mean age male SD
Patients
Controls
145
43 (30%)
102 (70%)
111 (76%)
34 (24%)
39.2 14.8
40.5 14.1
36.1 16.2
342
146 (43%)
196 (57%)
279 (82%)
63 (18%)
41.3 13.1
39.2 13.4
44.1 12.1
RHD patients
RFo patients
103
25 (24.3%)
78 (75.8%)
86 (83.5%)
17 (16.5%)
46.4 10.8
46.1 10.7
47.2 11.1
42
18 (42.8%)
24 (57.1%)
25 (59.5%)
17 (40.5%)
21.6 6.0
22.3 5.8
20.7 6.3
OR [95% CI]a
P valuea
OR [95% CI]b
P valueb
0.57 [0.370.86]
<0.0001
n.a.
n.a.
n.s.
n.s.
n.s.
n.s.
n.a.
n.a.
n.a.
n.a.
OR [95% CI]a
P valuea
OR [95% CI]b
P valueb
0.43 [0.20.91]
0.028
n.s.
n.s.
0.29 [0.130.65]
1.71 [1.332.19]
0.003
<0.0001
n.s.
1.72 [1.322.24]
n.s.
<0.0001
n.s.: not signicant; n: number of individuals; n.a.: not applicable; RHD: rheumatic heart disease; RFo: rheumatic fever only; SD: standard deviation.
a
OR and P values obtained by univariate binary logistic regression.
b
OR and P values corrected by multivariate binary logistic regression.
distribution with ShapiroWilk test. Since they did not follow normality, distributions were compared with nonparametric Mann
Whitney or KruskalWallis tests and correlations were evaluated
with Spearmans rank correlation coefcient, using the GraphPad
Prism 5.01 software. Associations were analyzed with two-tailed
exact Fisher test using SISA (http://www.quantitativeskills.com/
sisa). They were corrected for associated demographic factors
using logistic regression with the software package STATA 9.2.
Two-tailed P values 65% were considered signicant.
3. Results
3.1. MASP2 polymorphisms
MASP2 genotype distributions were in HardyWeinberg
equilibrium and were homogeneous between patients and
controls. Among the 11 SNPs investigated, two of them p.377A
and p.439H were negatively associated with the disease (Table 2).
Both were associated with protection against RF (6/290 or 2.1% in
patients vs. 38/684 or 5.6% in controls, P = 0.02, OR = 0.36 [95%
CI = 0.150.86]) and against RHD (3/206 or 1.5% in RHD vs. 38/
684 or 5.6% in controls, P = 0.01, OR = 0.25 [95% CI = 0.080.82]).
MASP2 genotypes containing SNPs p.377A and p.439H were also
associated with protection against RF per se (6/145 or 4.1% in
patients vs. 38/342 or 11.1% in controls, P = 0.02, OR = 0.34 [95%
CI = 0.140.83]). The allelic association remained after correction
for sex distribution (P = 0.02, OR = 0.35 [95% CI = 0.140.85]). The
p.377A and p.439H polymorphisms occur in strong linkage
disequilibrium with the other investigated polymorphisms,
imbedded in two haplotypes: 2A2-l [AG] and 1C2-l [AG],
respectively (Table 3).
In contrast to them, haplotypes that share the intron 9 exon
12 CDVR polymorphisms (1C1-l [AG], 1A [AG], 1A [GA] and 2A1
Table 2
Minor allele frequencies (%) of MASP2 SNPs.
Reference:
NP_006601.2
aminoacid
Protein
domain
Protein
levelsa
Protein functionb
Patients
(n = 290)
Controls
(n = 684)
RHD
patients
(n = 206)
RFo
patients
(n = 84)
rs7548659
Promoter g.4847A>C
rs61735600 Exon 3
g.5557G>A
rs72550870 Exon 3
g.5620A>G
n.a.
p.R99Q
p.D120G
n.a.
CUB1
CUB1
Variable
P600 ng/ml
6200 ng/ml
100 (34.5)
0
5 (1.7)
215 (31.4)
6 (0.9)
8 (1.2)
76 (36.9)
0
4 (1.9)
24 (28.6)
0
1 (1.2)
1
2
2
3
3
3
4
rs56392418
rs2273344
rs9430347
rs17409276
rs12711521
rs2273346
rs12085877
Exon 3
Intron 4
Intron 5
Intron 9
Exon 10
Exon 10
Exon 12
g.5638C>T
g.7164A>G
g.7441G>A
g.21081C>T
g.21370G>T
g.21389T>C
g.24599G>A
p.P126L
n.a.
n.a.
n.a.
p.Y371D
p.V377A
p.R439H
CUB1
n.a.
n.a.
n.a.
CCP2
CCP2
SP
6200 ng/ml
P600 ng/ml
P600 ng/ml
P600 ng/ml
Variable
6200 ng/ml
6200 ng/ml
6 (2.1)
62 (21.4)
62 (21.4)
51 (17.6)
81 (27.9)
6 (2.1)
0
9 (1.3)
124 (18.1)
124 (18.1)
103 (15.1)
183 (26.8)
32 (4.7)
6 (0.9)
6 (2.9)
44 (21.4)
44 (21.4)
36 (17.5)
61 (29.6)
3 (1.5)
0
0
18 (21.4)
18 (21.4)
15 (17.9)
20 (23.8)
3 (3.6)
0
rs1782455
Exon 12
g.24762T>C
p.S493=
SP
Variable
n.a.
Normal
Cannot bind MBL,
cannot activate C4
Normal
n.a.
n.a.
n.a.
Normal
Normal
Binds MBL but
does not
autoactivate,
cannot activate C4
n.a. (synonymous)
74 (25.5)
149 (21.8)
57 (27.7)
17 (20.2)
Haplotype
block
dbSNP
1
1
1
Gene
region
Reference:
NG007289.1
alleles
dbSNP: database of single nucleotide polymorphisms; n: number of chromosomes; RHD: rheumatic heart disease; RFo: rheumatic fever only; n.a.: not applicable; CUB1: C1r/
C1s, UegF and bone morphogenetic protein 1; CCP2: complement control protein; SP: serine protease. In bold: alleles negatively associated with the disease. Allele
nomenclature was italicized, as recommended by the HGVS.
a
Reported effect of homozygosity of exonic minor alleles [1619] and intronic minor alleles [18,19].
b
Reported results from in vitro studies [17]. Allele frequencies are given as percentages in parentheses. Haplotype blocks: (1) promoter variant at nucleotide position
1945560 and three amino acid variants due to nucleotide substitutions at codons 99, 120 and 126 (ARDP, ARGP, CRDP, CQDP, CRDL); (2) intron 4 and 5 variants (AG, GA, GG),
(3) intron 9 and two amino acid variants at codons 371 and 377 (CDA, CDV, TDV), (4) amino acid variant at codon 439 and a synonymous variant at nucleotide position 24762
(RC, HC, RT).
1200
S.J.d.S. Catarino et al. / Human Immunology 75 (2014) 11971202
Table 3
MASP2 haplotype frequencies (%) in patients and controls.
Haplotypea
ARDP AG CYV RT
ARDP GA CYV RT
ARGP AG CYV RT
CQDP GA TDV RC
CRDP AG CYV RT
CRDP AG TDV RC
CRDP GA CYV RT
CRDP GA TDV RC
ARDP AG TDV RC
Protective haplotypes
CRDL AG CDV HC
CRDP AG CDA RT
Susceptibility haplotypes
CRDL AG CDV RC
CRDP AG CDV RC
CRDP AG CDV RT
CRDP GA CDV RC
Phylogenetic
nomenclatureb
Protein Levelsc
2B2A-i [AG]
2B2A-i [GA]
2B2B-l [AG]
1B2-h [GA]
2B1-i [AG]
1B1-h [AG]
2B1-i [GA]
1B1-h [GA]
2B2A-i.1B1-h [AG]
>200 < 400 ng/ml
>400 < 600 ng/ml
6200 ng/ml
P600 ng/ml
>200 < 400 ng/ml
P400 ng/ml
>400 < 600 ng/ml
P600 ng/ml
>400 < 600 ng/ml
Normal
Normal
Decient
Normal
Normal
Normal
Normal
Normal
Normal
1C2-l [AG]
2A2-l [AG]
6200 ng/ml
6200 ng/ml
Decient
Normal
1C1-l [AG]
1A [AG]
2A1 [AG]
1A [GA]
6200 ng/ml
Variable
Variable
Variable
Normal
Normal
Normal
Normal
C4
activation
Patients
(n = 290)
Controls
(n = 684)
RHD patients
(n = 206)
RFo patients
(n = 84)
181 (62.4)
3 (1.0)
5 (1.7)
0
13 (4.5)
2 (0.7)
7 (2.4)
48 (16.6)
1 (0.3)
453 (66.2)
7 (1.0)
8 (1.2)
6 (0.9)
22 (3.2)
5 (0.7)
11 (1.6)
91 (13.3)
1 (0.1)
124 (60.2)
2 (1.0)
4 (1.9)
0
11 (5.3)
2 (1.0)
4 (1.9)
34 (16.5)
0
57 (67.9)
1 (1.2)
1 (1.2)
0
2 (2.4)
0
3 (3.6)
14 (16.7)
1 (1.2)
0
6 (2.1)
6 (0.9)
28 (4.7)
0
3 (1.5)
0
3 (3.6)
6 (2.1)
13 (4.5)
1 (0.3)
4 (1.4)
3 (0.4)
28 (4.1)
2 (0.3)
9 (1.3)
6 (2.9)
11 (5.3)
1 (0.5)
4 (1.9)
0
2 (2.4)
0
0
Haplotype nomenclature was italicized, as recommended by the HGVS. Haplotype frequencies are given as percentages in parentheses.
n: number of chromosomes, RHD: rheumatic heart disease; RFo: rheumatic fever only.
a
Each haplotype block is separated by a space. First haplotype block include variants from the promoter to exon 3, second block include polymorphisms in intron 4 and 5,
third block include variants in intron 9 and exon 10, fourth block include variants in exon 12. For nonsynonimous SNPs, aminoacid changes are indicated, e.g. CDV means a
cytosine (C) at position 21081 in intron 9, followed by two closely located nucleotide substitutions encoding asparagine (D) at residue 371 and valine (V) at residue 377 of the
protein.
b
In the alphanumerical system of the phylogenetic nomenclature, rst clade is given by a number, followed by as many letters and numbers as branches/lineages in the
tree [39]. In the case of MASP2, the system was added by a l for haplotypes generating low MASP-2 levels, i for haplotypes generating intermediate MASP-2 levels, h
for haplotypes generating high MASP-2 levels [18]. It was also added by the alleles in introns 4 and 5 (within brackets), which are not in linkage disequilibrium with all
other investigated SNPs [19]. Recombinant haplotypes are given by the names of the possible parental haplotypes, separated by a dot. Clade 1 haplotypes share g.24762C in
exon 12: 1A (most ancient), 1B1-h and 1B2-h (sharing g.21081T), 1C1-l and 1C2-l (sharing p.126L). Five other haplotypes present g.24762T in exon 12 and belong to clade 2:
2A1, 2A2-l (with the p.377A variant), 2B1-I, the very common 2B2A-i and 2B2B-l (with the p.120G variant).
c
Reported effect of homozygous haplotypes [18,19].
d
Reported results from in vitro studies. The effect of a recombinant protein with both p.126L and p.439H residues, encoded by 1C2-l, is unknown, although a protein with
p.439H is unable to bind MBL [17].
[AG]) increased the susceptibility to RHD among RF patients
(22/206 or 10.7% in RHD patients vs. 2/84 or 2.4% in RFo patients,
P = 0.02, OR = 4.9 [95% CI = 1.1321.34]). This association remained
after correction for age, which was the only demographic factor
associated with RHD in comparison to RFo patients (P = 0.02).
and ethnic group: P < 0.0001, OR = 0.20 [95% CI = 0.090.47])
(Fig. 1). The difference remained after comparing controls and
RHD, but not RFo patients, and was independent of sex, age and
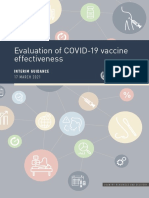
3.2. MASP-2 levels
Patients presented lower MASP-2 levels than controls, with
medians 252.8 and 313.9 ng/ml, respectively (corrected for age
Fig. 1. MASP-2 levels in patients and controls. Medians and minmax ranges are
shown. MASP-2 levels were compared with MannWhitney test.
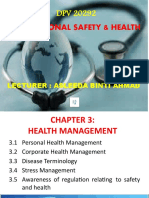
Fig. 2. MASP-2 levels are associated with MASP2 genotypes. Medians and minmax
ranges are shown. MASP-2 levels were compared with KruskalWallis test. h:
genotypes with haplotypes containing the sufx h (h/h and h/i), ii: homozygote
genotypes with haplotypes containing the sufx i (i/i), l: genotypes with haplotypes
containing the sufx l (l/l and l/i). We excluded 41 individuals (22 controls and 19
patients) due to ambiguous genotypephenotype associations: seven were h/l
heterozygotes and the others presented haplotypes not formerly associated with
MASP-2 levels [18,19].
S.J.d.S. Catarino et al. / Human Immunology 75 (2014) 11971202
ancestry (P < 0.0001, OR = 0.11 [95% CI = 0.030.42]). MASP-2 levels, nevertheless, did not differ between RHD and RFo patients
(medians 254.9 and 241.6 ng/ml, respectively).
We further conrmed previously reported associations of
MASP2 haplotypes with MASP-2 levels, in both controls and
patients. This was evident comparing genotypes with haplotypes
reportedly associated with high MASP-2 concentrations (equal or
higher than 600 ng/ml, produced by haplotypes containing the sufx h: h/h and h/i), intermediate concentrations (between 200 and
600 ng/ml, produced by haplotype with the sufx i: i/i) and low
concentrations (less than or equal to 200 ng/ml, produced by
haplotype with the sufx l: l/l and l/i). As expected, the genotypephenotype association was more conspicuous in the control
group (Fig. 2). Interestingly, we did not identify p.99Q among
patients, which is a variant known to be associated with high
MASP-2 levels (0.9% in controls, not signicant) (Table 2).
4. Discussion
Rheumatic fever is still a disease with great impact on the public
health system of developing countries, where disease prevalence is
high and expenses with cardiac surgeries, expressive [28]. Thus,
attempts to elucidate the autoimmune and physiological mechanisms in this condition are important. Protection against invading
pathogens relies on complex interactions between the genetically
controlled innate and adaptive immune responses. In fact, several
polymorphisms in genes that encode molecules involved in both
innate and adaptive immune responses were shown to contribute
to RF and RHD susceptibility [29]. The activation of complement
cascade provides a rst line of defense against Streptococcus pyogenes infections. Due to its importance in clearance of rheumatic etiological agents as well as in disposal of apoptotic bodies and
potential autoimmune initiators, deciencies of components of
the lectin pathway have been found to increase susceptibility and
modulate severity of most rheumatic disorders [30].
This is the rst study to investigate a number of polymorphisms
encompassing the whole MASP2 gene as well as related haplotypes
and MASP-2 levels in patients with RF and RHD. We conrmed
previously noticed associations between MASP2 polymorphisms/
haplotypes and MASP-2 levels [1619] and the absence of an association with the p.D120G polymorphism [26,31]. MASP-2 levels
were lower in patients, than in controls. These patients were the
same formerly found with higher MBL levels [32]. Higher MBL
and lower MASP-2 levels are consistent with MASP-2 consumption
due to intense MBL-driven complement activation. Lower MASP-2
levels were also found in patients with myocardial infarction
compared to controls, suggesting an involvement of the protein
in complement activation following ischemia and myocardial
necrosis [33]. On the other hand, higher MASP-2 levels were
associated with improved survival in patients with hematologic
malignancies, specically lymphoma [34].
We further found an association of two SNPs (p.V377A and
p.R439H) known to cause low MASP-2 levels [16,17], with protection against RF and RHD. p.R439H was reported also to protect
against placental malaria [21]. In contrast, these SNPs were
recently described to increase the susceptibility to leprosy [19].
The contrasting associations are not surprising, since MASP-2 modulates phagocytosis, complement and coagulation cascades, each
exerting a different role in the susceptibility to infectious and autoimmune diseases [8,16,17]. Furthermore, the association between
variants leading to low protein levels and protection against RF
has been formerly found for MBL2 [35,36], but not for FCN2 [37].
The low basal concentrations of MBL and MASP-2 correspond to
a lower capacity of complement activation, due to structural variants as p.52C, p.54D and p.57E in MBL2 and p.439H in MASP2 [30].
1201
This reinforces our suggestion that complement activation through
the lectin pathway promote the inammatory response and subsequent tissue damage in rheumatic fever disease.
On the other hand, MASP2 CDVR haplotypes, encompassing
g.1961795C, p.371D, p.377V and p.439R variants, where associated
with an almost ve times increased risk to RHD. They generate
varying MASP-2 levels and are phylogenetically related to the most
ancestral MASP2 haplotype [18]. These haplotypes probably harbor
other polymorphisms not investigated in this study, which could
contribute to the disease. Interestingly, the p.371D variant was also
reported to increase susceptibility to HCV infection [20], D/D
homozygotes were associated with bacterial infections after orthotopic liver transplantation [22] and the CD haplotype was found
associated with susceptibility to chagasic cardiomyopathy [23].
Although cardiac commitments in Chagas disease and RHD cannot
be compared, both may share autoimmune etiology [38].
In conclusion, the effects of MASP2 polymorphisms on protein
serum levels and functional efciency may modulate susceptibility
to RF. MASP-2 levels were lower in patients, which may reect
protein consumption due to complement activation. This is in
agreement with our former results regarding MBL protein and
polymorphisms of the MBL2 gene. MASP2 gene polymorphisms
and protein levels seem to play an important role in the development of RF and establishment of RHD.
Funding
This work was supported by CNPq - Brazil (Conselho Nacional
de Desenvolvimento Cientco e Tecnolgico) and CAPES - Brazil
(Coordenao de Aperfeioamento de Pessoal de Nvel Superior).
Acknowledgments
We gratefully acknowledge the patients for their participation
in this study and thank the staff of the Laboratrio de Imunopatologia Molecular HC/UFPR for their assistance.
References
[1] Chang C. Cutting edge issues in rheumatic fever. Clin Rev Allergy Immunol
2011:125.
[2] Burke RJ, Chang C. Diagnostic criteria of acute rheumatic fever. Autoimmun
Rev 2014;13:5037.
[3] Guilherme L, Kohler K, Kalil J. Rheumatic heart disease: mediation by complex
immune events. Adv Clin Chem 2011;53:3150.
[4] Tibazarwa K, JA V, Mayosi B. Incidence of acute rheumatic fever in the world: a
systematic review of population-based studies. Heart 2008;94:153440.
[5] Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A
streptococcal diseases. Lancet Infect Dis 2005;5:68594.
[6] Kumar RK, Tandon R. Rheumatic fever & rheumatic heart disease: the last
50 years. Indian J Med Res 2013;137:64358.
[7] Barbosa P, Muller R, Latado A, Achutti A, Ramos A, Weksler C. Diretrizes
brasileiras para o diagnstico, tratamento e preveno da febre reumtica. Arq
Bras Cardiol 2009;93:118.
[8] Mayilyan KR. Complement genetics, deciencies, and disease associations.
Protein Cell 2012;3:48796.
[9] Stger S, Alexander J, Kirby AC, Botto M, Van Rooijen N, Smith DF, et al. Natural
antibodies and complement are endogenous adjuvants for vaccine-induced
CD8+ T-cell responses. Nat Med 2003;9:128792.
[10] Degn SE, Jensenius JC, Thiel S. Disease-causing mutations in genes of the
complement system. Am J Hum Genet 2011;88:689705.
[11] Matsushita M, Endo Y, Fujita T. Structural and functional overview of the lectin
complement pathway: its molecular basis and physiological implication. Arch
Immunol Ther Exp (Warsz) 2013;61:27383.
[12] Stover CM, Thiel S, Thelen M, Lynch NJ, Vorup-Jensen T, Jensenius JC, et al. Two
constituents of the initiation complex of the mannan-binding lectin activation
pathway of complement are encoded by a single structural gene. J Immunol
1999;162:348190.
[13] Thiel S. Complement activating soluble pattern recognition molecules with
collagen-like regions, mannan-binding lectin, colins and associated proteins.
Mol Immunol 2007;44:387588.
[14] Laursen I, Thielens N, Christiansen M, Houen G. MASP interactions with
plasma-derived MBL. Mol Immunol 2012;52:7987.
1202
S.J.d.S. Catarino et al. / Human Immunology 75 (2014) 11971202
[15] Stengaard-Pedersen K, Thiel S, Gadjeva M, Mller-Kristensen M, Srensen R,
Jensen LT, et al. Inherited deciency of mannan-binding lectin-associated
serine protease 2. N Engl J Med 2003;349:55460.
[16] Thiel S, Steffensen R, Christensen IJ, Ip WK, Lau YL, Reason IJM, et al. Deciency
of mannan-binding lectin associated serine protease-2 due to missense
polymorphisms. Genes Immun 2007;8:15463.
[17] Thiel S, Kolev M, Degn S, Steffensen R, Hansen AG, Ruseva M, et al.
Polymorphisms in mannan-binding lectin (MBL)-associated serine protease 2
affect stability, binding to MBL, and enzymatic activity. J Immunol
2009;182:293947.
[18] Boldt ABW, Grisbach C, Steffensen R, Thiel S, Kun JFJ, Jensenius JC, et al.
Multiplex sequence-specic polymerase chain reaction reveals new MASP2
haplotypes associated with MASP-2 and MAp19 serum levels. Hum Immunol
2011;72:75360.
[19] Boldt ABW, Goeldner I, Stahlke ERS, Thiel S, Jensenius JC, de Messias-Reason
IJT. Leprosy association with low MASP-2 levels generated by MASP2
haplotypes and polymorphisms anking MAp19 exon 5. PLoS One
2013;8:e69054.
[20] Tulio S, Faucz FR, Werneck RI, Olandoski M, Alexandre RB, Boldt ABW, et al.
MASP2 gene polymorphism is associated with susceptibility to hepatitis C
virus infection. Hum Immunol 2011;72:9125.
[21] Holmberg V, Onkamo P, Lahtela E, Lahermo P, Bedu-Addo G, Mockenhaupt FP,
et al. Mutations of complement lectin pathway genes MBL2 and MASP2
associated with placental malaria. Malar J 2012;11:61.
[22] De Rooij B-JF, van Hoek B, ten Hove WR, Roos A, Bouwman LH, Schaapherder
AF, et al. Lectin complement pathway gene prole of donor and recipient
determine the risk of bacterial infections after orthotopic liver transplantation.
Hepatology 2010;52:110010.
[23] Boldt ABW, Luz PR, Messias-Reason IJT. MASP2 haplotypes are associated with
high risk of cardiomyopathy in chronic Chagas disease. Clin Immunol
2011;140:6370.
[24] Goeldner I, Skare T, Boldt ABW, Nass FR, Messias-Reason IJ, Utiyama SR.
Association of MASP-2 levels and MASP2 gene polymorphisms with
rheumatoid arthritis in patients and their relatives. PLoS One 2014;9:e90979.
[25] Dajani AS, Ayoub E, Bierman FZ, Bisno AL, Denny FW, Durack DT, et al.
Guidelines for the diagnosis of rheumatic fever: Jones criteria, 1992 update.
JAMA 1992;268:206973.
[26] Schafranski MD, Pereira Ferrari L, Scherner D, Torres R, de Messias-Reason IJ.
Functional MASP2 gene polymorphism in patients with history of rheumatic
fever. Hum Immunol 2008;69:414.
[27] Excofer L, Lischer HEL. Arlequin suite ver 3.5: a new series of programs to
perform population genetics analyses under Linux and Windows. Mol Ecol
Resour 2010;10:5647.
[28] Guilherme L, Kalil J. Rheumatic heart disease: molecules involved in valve
tissue inammation leading to the autoimmune process and anti-S. pyogenes
vaccine. Front Immunol 2013;4:352.
[29] Guilherme L, Khler KF, Kalil J. Rheumatic heart disease: genes, inammation
and autoimmunity. Rheumatol Curr Res 2012;S4(001):15.
[30] Boldt ABW, Goeldner I, De Messias-Reason IJT. Relevance of the lectin pathway
of complement in rheumatic diseases. Adv Clin Chem 2012;56:10553.
[31] Ramasawmy R, Spina GS, Fae KC, Pereira AC, Nisihara R, Messias Reason IJ,
et al. Association of mannose-binding lectin gene polymorphism but not of
mannose-binding serine protease 2 with chronic severe aortic regurgitation of
rheumatic etiology. Clin Vaccine Immunol 2008;15:9326.
[32] Schafranski MD, Pereira Ferrari L, Scherner D, Torres R, Jensenius JC, de
Messias-Reason IJ. High-producing MBL2 genotypes increase the risk of acute
and chronic carditis in patients with history of rheumatic fever. Mol Immunol
2008;45:382731.
[33] Zhang M, Hou YJ, Cavusoglu E, Lee DC, Steffensen R, Yang L, et al. MASP-2
activation is involved in ischemia-related necrotic myocardial injury in
humans. Int J Cardiol 2013;166:499504.
[34] Zehnder A, Fisch U, Hirt A, Niggli FK, Simon A, Ozsahin H, et al. Prognosis in
pediatric hematologic malignancies is associated with serum concentration of
mannose-binding lectin-associated serine protease-2 (MASP-2). Pediatr Blood
Cancer 2009;53:537.
[35] Schafranski MD, Stier A, Nisihara R, Messias-Reason IJT. Signicantly increased
levels of mannose-binding lectin (MBL) in rheumatic heart disease: a
benecial role for MBL deciency. Clin Exp Immunol 2004;138:5215.
[36] Messias Reason IJ, Schafranski MD, Jensenius JC, Steffensen R. The association
between mannose-binding lectin gene polymorphism and rheumatic heart
disease. Hum Immunol 2006;67:9918.
[37] Messias-Reason IJ, Schafranski MD, Kremsner PG, Kun JFJ. Ficolin 2 (FCN2)
functional polymorphisms and the risk of rheumatic fever and rheumatic heart
disease. Clin Exp Immunol 2009;157:3959.
[38] McLean B, Oudit GY. Role of autoimmunity in heart disease: is Chagas heart
disease the denitive proof? Can J Cardiol 2014;30:2679.
[39] Nebert DW. Proposal for an allele nomenclature system based on the
evolutionary divergence of haplotypes. Hum Mutat 2002;20:46372.
Вам также может понравиться
- tmpF178 TMPДокумент15 страницtmpF178 TMPFrontiersОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Tmpa077 TMPДокумент15 страницTmpa077 TMPFrontiersОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Tmp1a96 TMPДокумент80 страницTmp1a96 TMPFrontiersОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- tmpE3C0 TMPДокумент17 страницtmpE3C0 TMPFrontiersОценок пока нет
- tmp998 TMPДокумент9 страницtmp998 TMPFrontiersОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- tmp27C1 TMPДокумент5 страницtmp27C1 TMPFrontiersОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- tmp3656 TMPДокумент14 страницtmp3656 TMPFrontiersОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- tmp97C8 TMPДокумент9 страницtmp97C8 TMPFrontiersОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- tmp96F2 TMPДокумент4 страницыtmp96F2 TMPFrontiersОценок пока нет
- tmpA7D0 TMPДокумент9 страницtmpA7D0 TMPFrontiersОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Soal Anbk English Dan PKNДокумент14 страницSoal Anbk English Dan PKNRahma Aprilia65Оценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Kode Icd 10Документ29 страницKode Icd 10Zakia NisakОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- TonsilofaringitisДокумент1 страницаTonsilofaringitisFadhli Rajif TangkeОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Worksheet 1Документ3 страницыWorksheet 1Joewellyn LimОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- RelianceДокумент13 страницRelianceSamir DesaiОценок пока нет
- Assignment On Designing A Communication Campaign For Mexico About HIVДокумент11 страницAssignment On Designing A Communication Campaign For Mexico About HIVxhuvo50% (2)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Drug Study (Romel Cruz Hospital)Документ35 страницDrug Study (Romel Cruz Hospital)Djoan SamontañezОценок пока нет
- Nursing Seminar 1 SAS Session 16Документ8 страницNursing Seminar 1 SAS Session 16ZiaОценок пока нет
- CICE Sample MCQsДокумент6 страницCICE Sample MCQsNuredin IbrahimОценок пока нет
- CONSENT FORM Kap Dengue LatestДокумент6 страницCONSENT FORM Kap Dengue Latestfairus_fz821575Оценок пока нет
- MAS110 - Week 1 - Infection Control Worksheet 2Документ4 страницыMAS110 - Week 1 - Infection Control Worksheet 2geonikawilliamsОценок пока нет
- 05-S-2019 Dengue Ordinance of Barangay San CarlosДокумент6 страниц05-S-2019 Dengue Ordinance of Barangay San CarlosRonel Rosal MalunesОценок пока нет
- SOP Validation Kits Veterinary DiagnosisДокумент26 страницSOP Validation Kits Veterinary DiagnosishumusdelombrizОценок пока нет
- WHO 2019 nCoV Vaccine Effectiveness Measurement 2021.1 EngДокумент70 страницWHO 2019 nCoV Vaccine Effectiveness Measurement 2021.1 EngChio MoranteОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Ujian Bhasa InggrisДокумент41 страницаUjian Bhasa InggrisErna DekaОценок пока нет
- Public Health LawsДокумент7 страницPublic Health LawsijonkjnkjОценок пока нет
- The Virus Misconception Part 1Документ14 страницThe Virus Misconception Part 1Zdravlje MarijaS100% (1)
- Objectives 3Документ4 страницыObjectives 3sibugan300Оценок пока нет
- Aseptic Meningitis: Exams and TestsДокумент8 страницAseptic Meningitis: Exams and TestsJoylyn Sagon VergaraОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- MumpsДокумент2 страницыMumpsArjunJainОценок пока нет
- Revised Crop Diseases - FormattedДокумент98 страницRevised Crop Diseases - FormattedMona ElsayedОценок пока нет
- Domingo - Jose Carlo - 3CMT - MT6320LabActivityДокумент8 страницDomingo - Jose Carlo - 3CMT - MT6320LabActivityJC DomingoОценок пока нет
- ChiroRab Press Release Nov 13 2019 PDFДокумент2 страницыChiroRab Press Release Nov 13 2019 PDFsr bОценок пока нет
- Memorandum: Rule 198 of WBSR, PTДокумент2 страницыMemorandum: Rule 198 of WBSR, PTMd. Sahir KhanОценок пока нет
- Occupational Safety & Health: Lecturer: Asleeda Binti AhmadДокумент23 страницыOccupational Safety & Health: Lecturer: Asleeda Binti AhmadIzzad FikriОценок пока нет
- Fiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1Документ133 страницыFiji Communicable Disease Surveillance and Outbreak Response Guidelines 2016 1roddy narayanОценок пока нет
- Virology GuideДокумент30 страницVirology GuideBianca QuijijeОценок пока нет
- PDS - Metazolone-FM - Ver 2.0Документ1 страницаPDS - Metazolone-FM - Ver 2.0Rama KrishnanОценок пока нет
- (From The Department of Bacteriology, School of Medicine, American University of Beirut, Beirut, Syria) Plates 64 A CD 65Документ18 страниц(From The Department of Bacteriology, School of Medicine, American University of Beirut, Beirut, Syria) Plates 64 A CD 65diantinurwindaОценок пока нет
- Dextrocardia BAVДокумент3 страницыDextrocardia BAVchiapas52Оценок пока нет