Вам также может понравиться
- For PrintingДокумент1 страницаFor PrintingHowell YapОценок пока нет
- CPG Management of Dengue Infection in Adults (Revised 2nd Edition)Документ68 страницCPG Management of Dengue Infection in Adults (Revised 2nd Edition)umiraihana1Оценок пока нет
- PrayerДокумент1 страницаPrayerHowell YapОценок пока нет
- Opd Meds Jgej PDFДокумент4 страницыOpd Meds Jgej PDFKaty SanchezОценок пока нет
- CPG Pcap 2012 PDFДокумент54 страницыCPG Pcap 2012 PDFroshmae67% (3)
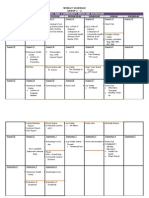
- FM Rotation Weekly Schedule Group C-2Документ2 страницыFM Rotation Weekly Schedule Group C-2Howell YapОценок пока нет
- Therapeutic IndexДокумент8 страницTherapeutic IndexHowell YapОценок пока нет
- 8356Документ8 страниц8356Howell YapОценок пока нет
- Opd Meds Jgej PDFДокумент4 страницыOpd Meds Jgej PDFKaty SanchezОценок пока нет
- Management of Febrile SeizuresДокумент13 страницManagement of Febrile SeizuresfitriohpОценок пока нет
- Febrile Seizure GuidelineДокумент1 страницаFebrile Seizure GuidelinesmileyginaaОценок пока нет
- Compiled Case Study-LenovoДокумент24 страницыCompiled Case Study-LenovoHowell Yap100% (2)
- Local AnestheticsДокумент3 страницыLocal Anestheticsravi98195Оценок пока нет
- W10 Water, Vitamins & MineralsДокумент37 страницW10 Water, Vitamins & MineralsHowell YapОценок пока нет
- Henoch SCH NleinДокумент42 страницыHenoch SCH NleinHowell YapОценок пока нет
- NДокумент1 страницаNHowell YapОценок пока нет
- FINAL Outcome Community Grand ProjectДокумент4 страницыFINAL Outcome Community Grand ProjectHowell YapОценок пока нет
- NДокумент6 страницNHowell YapОценок пока нет
- (FCM3) G7-8. ProjectPlanning - maternalReproductiveHealthДокумент11 страниц(FCM3) G7-8. ProjectPlanning - maternalReproductiveHealthHowell YapОценок пока нет
- LUCAS vs TUAÑO CaseДокумент2 страницыLUCAS vs TUAÑO CaseHowell YapОценок пока нет
- For Asthma and COPDДокумент14 страницFor Asthma and COPDHowell YapОценок пока нет
- 3b Ctc#05 Malaria 06.27.14edited2Документ28 страниц3b Ctc#05 Malaria 06.27.14edited2Howell YapОценок пока нет
- To DoДокумент1 страницаTo DoHowell YapОценок пока нет
- GitДокумент5 страницGitHowell YapОценок пока нет
- FCДокумент1 страницаFCHowell YapОценок пока нет
- Community Immersion Program FormatДокумент2 страницыCommunity Immersion Program FormatHowell YapОценок пока нет
- AnthraxДокумент3 страницыAnthraxHowell YapОценок пока нет
- UntitledДокумент1 страницаUntitledHowell YapОценок пока нет
- Overview of Carbohydrate Metabolism PathwaysДокумент3 страницыOverview of Carbohydrate Metabolism PathwaysHowell YapОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Manufacturing process F1 racing car proposalДокумент4 страницыManufacturing process F1 racing car proposalFirdaus IliasОценок пока нет
- Foot and Ankle ANATOMY PDFДокумент80 страницFoot and Ankle ANATOMY PDFMark JayОценок пока нет
- Physics I Practice Problems Set 2 1Документ17 страницPhysics I Practice Problems Set 2 1killerspikeОценок пока нет
- Bowling Score SheetДокумент2 страницыBowling Score SheetMusadya100% (2)
- 722.9 Tranmission ServiceДокумент3 страницы722.9 Tranmission ServiceKISKACОценок пока нет
- Paracord Monkeys Fist 1Документ9 страницParacord Monkeys Fist 1dildim familyОценок пока нет
- EVOBET88 Situs Judi Slot Online Gacor Dan Agen Judi Bola PDFДокумент1 страницаEVOBET88 Situs Judi Slot Online Gacor Dan Agen Judi Bola PDFArrafi FahrezaОценок пока нет
- Ov2640 V1.2 SCHДокумент2 страницыOv2640 V1.2 SCHw2714554966Оценок пока нет
- Consolidated Grading Sheet 3rd Quarter, 2nd Sem SY. 2018-2019 TVL 12 AДокумент42 страницыConsolidated Grading Sheet 3rd Quarter, 2nd Sem SY. 2018-2019 TVL 12 AEL FuentesОценок пока нет
- Sci 8 L5 - Kinetic EnergyДокумент12 страницSci 8 L5 - Kinetic EnergyTorres Jhon Chriz GabrielОценок пока нет
- Automotive PlatformsДокумент13 страницAutomotive PlatformsEd Ri71% (7)
- Handball Basics PDFДокумент13 страницHandball Basics PDFyunzhe hanОценок пока нет
- s570 t4 Maintenance ChartДокумент1 страницаs570 t4 Maintenance ChartEd VanegasОценок пока нет
- Unit 6 WKST 4 Answer Key RevДокумент3 страницыUnit 6 WKST 4 Answer Key RevTushar Raj83% (6)
- Barbell Sumo SquatДокумент2 страницыBarbell Sumo SquatDodaily workoutОценок пока нет
- Nombre ID Tilename InglésДокумент15 страницNombre ID Tilename InglésBruno Rodriguez100% (5)
- Siyensikula Script Not Yet CompleteДокумент2 страницыSiyensikula Script Not Yet CompleteJ AblangОценок пока нет
- Circ Mot-Grav Problems-08Документ2 страницыCirc Mot-Grav Problems-08S DASОценок пока нет
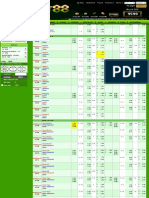
- Oaklawn Park: Daily Racing FormДокумент40 страницOaklawn Park: Daily Racing FormReille VanderОценок пока нет
- XilamДокумент3 страницыXilamkillian De MedeirosОценок пока нет
- Primal Paths: Path of IronДокумент1 страницаPrimal Paths: Path of IronI love you Evans PeterОценок пока нет
- A246E Automatic Transaxle Specs and Torque SettingsДокумент3 страницыA246E Automatic Transaxle Specs and Torque SettingsFSR14070% (1)
- Unit 2.1 Volleyball Lesson PlanДокумент8 страницUnit 2.1 Volleyball Lesson PlanMERI CRIS LEA GERA. CASABAОценок пока нет
- KamazДокумент12 страницKamazAl DiОценок пока нет
- 100 ESL Board Games PreviewДокумент10 страниц100 ESL Board Games PreviewAmrah AmrahovОценок пока нет
- 11 - SsangYong-Korando - 2012 - EN - US - Manual - de - Taller - Carroceria - 29fc2980d5Документ72 страницы11 - SsangYong-Korando - 2012 - EN - US - Manual - de - Taller - Carroceria - 29fc2980d5Mateus FumuassucaОценок пока нет
- Camel Pose Guide: Benefits, Instructions & VariationsДокумент8 страницCamel Pose Guide: Benefits, Instructions & VariationsToreØrnОценок пока нет
- Probability: A - B. C. DДокумент7 страницProbability: A - B. C. DabhanidharaОценок пока нет
- Gamak 2016-04-27-032451Документ103 страницыGamak 2016-04-27-032451NestramiОценок пока нет
- Sample PPE Request FormДокумент2 страницыSample PPE Request FormMaurice Balkissoon60% (15)