Вам также может понравиться
- Anxiety Disorder: A Self-Help Guide With Powerful Strategies for Overcoming Anxiety and Building Self-ConfidenceОт EverandAnxiety Disorder: A Self-Help Guide With Powerful Strategies for Overcoming Anxiety and Building Self-ConfidenceОценок пока нет
- Lecture 7 Lecture NotesДокумент5 страницLecture 7 Lecture NotesAafreen AhmedОценок пока нет
- AnxietyДокумент66 страницAnxietyMoses LaiОценок пока нет
- Anxiety and Phobia Workbook: 7 Self Help Ways How You Can Cure Them NowОт EverandAnxiety and Phobia Workbook: 7 Self Help Ways How You Can Cure Them NowРейтинг: 1.5 из 5 звезд1.5/5 (4)
- DSM 5 Categories Anxiety Related Disorders Into Three Categories AreДокумент10 страницDSM 5 Categories Anxiety Related Disorders Into Three Categories AreNeevalОценок пока нет
- Day 4 Disorders RVДокумент39 страницDay 4 Disorders RVapi-296712028Оценок пока нет
- Mental Disorder: Psychological (Or Mental) DisordersДокумент7 страницMental Disorder: Psychological (Or Mental) DisordersEsha MeherОценок пока нет
- Anxiety And Phobia Workbook: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Proven Cognitive MethodsОт EverandAnxiety And Phobia Workbook: A Guide to Breaking Free from Anxiety, Phobias, and Worry Using Proven Cognitive MethodsРейтинг: 5 из 5 звезд5/5 (24)
- Psychological Disorders: AP Psychology Mr. HollandДокумент20 страницPsychological Disorders: AP Psychology Mr. Hollandyummywords1254Оценок пока нет
- EDMR Therapy: 2 Manuscripts in 1 - Harnessing Eye Movements for HealingОт EverandEDMR Therapy: 2 Manuscripts in 1 - Harnessing Eye Movements for HealingОценок пока нет
- Anxiety DisordersДокумент39 страницAnxiety DisordersAugene ToribioОценок пока нет
- IntroductionДокумент13 страницIntroductionPrakash MangaloreОценок пока нет
- Lesson 6. Emotional-Behavioral DisordersДокумент7 страницLesson 6. Emotional-Behavioral DisordersEdsel DivinagraciaОценок пока нет
- List of Psychological DisordersДокумент12 страницList of Psychological DisordersClaire TeoxonОценок пока нет
- Psychology 1 TestДокумент8 страницPsychology 1 TestCarlos HurtadoОценок пока нет
- Study On Anxiety DisorderДокумент18 страницStudy On Anxiety DisorderRRRОценок пока нет
- Anxiety Disorders: Moges Ayehu, MD, Psychiatrist Assistant Professor, HUCMHДокумент38 страницAnxiety Disorders: Moges Ayehu, MD, Psychiatrist Assistant Professor, HUCMHsoran muzeyinОценок пока нет
- Sned 4 Anxiety DisorderДокумент16 страницSned 4 Anxiety DisordervelardecrazelleОценок пока нет
- Biopsychology of Psychiatruc Disorders - PPTX Filename UTF 8biopsychology of Psychiatruc DisordersДокумент50 страницBiopsychology of Psychiatruc Disorders - PPTX Filename UTF 8biopsychology of Psychiatruc DisordersMary Claire BagioenОценок пока нет
- Anxiety DisorderДокумент56 страницAnxiety DisorderDr TNTОценок пока нет
- Coun 646 Research Paper FinalДокумент18 страницCoun 646 Research Paper FinalMaLinda DiTonnoОценок пока нет
- What Are Anxiety Disorders?: Portfolio Output No.13: Research On Anxiety Disorders/ DepressionДокумент5 страницWhat Are Anxiety Disorders?: Portfolio Output No.13: Research On Anxiety Disorders/ DepressionPrincess Villasis BaciaОценок пока нет
- Psychology Notes Chpt. 13Документ5 страницPsychology Notes Chpt. 13ChloeОценок пока нет
- Presented By:: Tony Bratko MSC, LPC, LisacДокумент30 страницPresented By:: Tony Bratko MSC, LPC, LisacMarlaОценок пока нет
- Anxiety Disorder NewДокумент48 страницAnxiety Disorder NewIndah Permata SariОценок пока нет
- Introduction To Psychology: PsychopathologyДокумент56 страницIntroduction To Psychology: PsychopathologyIqbal Baryar100% (1)
- Types and Symptoms of Common Psychiatric DisordersДокумент6 страницTypes and Symptoms of Common Psychiatric DisordersRanusha AnushaОценок пока нет
- Psychological DisordersДокумент46 страницPsychological DisordersanОценок пока нет
- Anxiety DisorderДокумент53 страницыAnxiety DisorderGene Espino TrajecoОценок пока нет
- Dissociative Identity Disorder, (Multiple Personality Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandDissociative Identity Disorder, (Multiple Personality Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsРейтинг: 1 из 5 звезд1/5 (1)
- Types of Anxiety DisorderДокумент5 страницTypes of Anxiety Disordernilda asmin100% (1)
- Types of Mental IllnessДокумент6 страницTypes of Mental IllnessArjiel San MansuganОценок пока нет
- How Psychological Health Affects Your Physical Health: Toxic People Are No Good For YouОт EverandHow Psychological Health Affects Your Physical Health: Toxic People Are No Good For YouОценок пока нет
- PSYCH101 Lecture 10-11 PsychopathologyДокумент80 страницPSYCH101 Lecture 10-11 PsychopathologyLucy YengОценок пока нет
- The Ultimate Guide to Supporting Someone with Mental Illness: Managing Mental HealthОт EverandThe Ultimate Guide to Supporting Someone with Mental Illness: Managing Mental HealthОценок пока нет
- Anxiety Disorder-1Документ14 страницAnxiety Disorder-1Naeem Khan AfridiОценок пока нет
- Media Research Into Mental IllnessДокумент5 страницMedia Research Into Mental IllnessLillie Tamara DrewettОценок пока нет
- Emotional DisturbanceДокумент37 страницEmotional DisturbanceAngelo MirabelОценок пока нет
- Semio MSE PCEM 3Документ34 страницыSemio MSE PCEM 3Leng BunthaiОценок пока нет
- Psychological Disorders 2016Документ40 страницPsychological Disorders 2016Jonah the mixerОценок пока нет
- Anxiety Disorders: Powerpoint Lecture Notes PresentationДокумент43 страницыAnxiety Disorders: Powerpoint Lecture Notes PresentationErsido SamuelОценок пока нет
- Disorders RushedДокумент40 страницDisorders Rushedapi-391411195Оценок пока нет
- Abnormal PsychologyДокумент11 страницAbnormal Psychologyannistafford04Оценок пока нет
- ReportДокумент4 страницыReportErna Lorn DelaCerna EspañolaОценок пока нет
- Human Behavior Mid TermДокумент9 страницHuman Behavior Mid Termrosendophil7Оценок пока нет
- Handout Chapter15Документ3 страницыHandout Chapter15BismahMehdiОценок пока нет
- Clinical PsychologyДокумент26 страницClinical PsychologyGURNOOR KAURОценок пока нет
- Steps of Nursing Process Pertinent Nursing Diagnosis, Outcomes Apply QSEN PrinciplesДокумент8 страницSteps of Nursing Process Pertinent Nursing Diagnosis, Outcomes Apply QSEN Principlesjustjesko0lОценок пока нет
- Psychological Disorders Lecture Notes PDFДокумент8 страницPsychological Disorders Lecture Notes PDFTANUIОценок пока нет
- Steps To Take For Mental Health And Happiness A complete Guide To Your Well BeingОт EverandSteps To Take For Mental Health And Happiness A complete Guide To Your Well BeingОценок пока нет
- Mental Health and Mental Disorder ReportДокумент6 страницMental Health and Mental Disorder ReportBonJovi Mojica ArtistaОценок пока нет
- Chapter 12 VocabДокумент8 страницChapter 12 VocabTaylor NebrijaОценок пока нет
- EmailДокумент1 страницаEmailюрий локтионовОценок пока нет
- Russell-AthleticДокумент28 страницRussell-Athleticюрий локтионовОценок пока нет
- Interconnected-WorldДокумент1 страницаInterconnected-Worldюрий локтионовОценок пока нет
- HSBC in ChinaДокумент3 страницыHSBC in Chinaюрий локтионов100% (1)
- Bolender-MemoДокумент2 страницыBolender-Memoюрий локтионовОценок пока нет
- 4 9 NotesДокумент1 страница4 9 Notesюрий локтионовОценок пока нет
- Shame, Pride and Eating Disorders PDFДокумент14 страницShame, Pride and Eating Disorders PDFhodmezevasarhelj100% (1)
- Eating Disorder StatisticsДокумент2 страницыEating Disorder Statisticsרוברטו מורןОценок пока нет
- Unit 1Документ66 страницUnit 1Izabela CzekajОценок пока нет
- Eating Disorder 1Документ18 страницEating Disorder 1Osuolale John MakanjuolaОценок пока нет
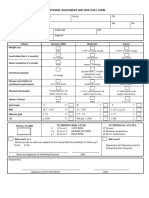
- 4 - Nutritional Assessment and Risk LevelДокумент1 страница4 - Nutritional Assessment and Risk LevelBok MatthewОценок пока нет
- D. Pour 2. B. Cherries 3. A. Bonus 4. A. Mysterious 5. C. PermanentДокумент4 страницыD. Pour 2. B. Cherries 3. A. Bonus 4. A. Mysterious 5. C. PermanentRMОценок пока нет
- Radio Show ScriptДокумент3 страницыRadio Show Scriptapi-531012846Оценок пока нет
- Abnormal Psychology Final Exam ReviewДокумент16 страницAbnormal Psychology Final Exam ReviewJimmy Nguyen90% (10)
- Effects of Treating Gender Dysphoria and Anorexia Nervosa in A Transgender Adolescent: Lessons LearnedДокумент4 страницыEffects of Treating Gender Dysphoria and Anorexia Nervosa in A Transgender Adolescent: Lessons LearnedCaio MayrinkОценок пока нет
- Beauty: Naomi Wolf The Beauty MythДокумент31 страницаBeauty: Naomi Wolf The Beauty MythUdiTa SinGh SalaRia100% (2)
- Anorexia Nervosa, Bulimia Nervosa, and Other Eating DisordersДокумент24 страницыAnorexia Nervosa, Bulimia Nervosa, and Other Eating DisordersEscobar JesusОценок пока нет
- PL100 Block 4 Study GuideДокумент31 страницаPL100 Block 4 Study GuidepwoerОценок пока нет
- NCM 117-Eating DisordersДокумент4 страницыNCM 117-Eating DisordersJa DimasОценок пока нет
- Sex Differences in Preferences For Ideal Female Body Shape: Health Care For Women InternationalДокумент12 страницSex Differences in Preferences For Ideal Female Body Shape: Health Care For Women InternationalLeonardo PinheiroОценок пока нет
- Positive Body ImageДокумент65 страницPositive Body Image3t1990100% (1)
- How Beauty Standards Came To BeДокумент3 страницыHow Beauty Standards Came To Beapi-537797933Оценок пока нет
- Is Emetophobia Different From Anorexia NervosaДокумент2 страницыIs Emetophobia Different From Anorexia Nervosascience&psychologyОценок пока нет
- Behavioral Models of Binge-Type EatingДокумент8 страницBehavioral Models of Binge-Type Eatingpechy83Оценок пока нет
- Social Media and Eating Disorder Psychopathology: A Systematic ReviewДокумент21 страницаSocial Media and Eating Disorder Psychopathology: A Systematic ReviewJosé Luis PsicoterapeutaОценок пока нет
- Food Addiction Can Lead To DeathДокумент1 страницаFood Addiction Can Lead To DeathFranco Jorge EnriqueОценок пока нет
- Chapter 8 Motivation and EmotionДокумент5 страницChapter 8 Motivation and EmotionMaricris GatdulaОценок пока нет
- Child Development Issues and Implications JournalДокумент26 страницChild Development Issues and Implications Journalapi-539933367Оценок пока нет
- Neuropsychiatric Effects of Caffeine: Anthony P. Winston, Elizabeth Hardwick & Neema JaberiДокумент8 страницNeuropsychiatric Effects of Caffeine: Anthony P. Winston, Elizabeth Hardwick & Neema JaberiMary TeohОценок пока нет
- Intimacy Anorexia: Healing The Hidden Addiction in Your MarriageДокумент20 страницIntimacy Anorexia: Healing The Hidden Addiction in Your Marriagedrdougweiss70% (10)
- Mental Health and WellДокумент9 страницMental Health and WellJohn rex QuintayoОценок пока нет
- Body Image and Mental Health: GlossaryДокумент6 страницBody Image and Mental Health: GlossarySalsa Dwi PutriОценок пока нет
- 334 MCQДокумент3 страницы334 MCQv_vijayakanth7656100% (1)
- Order 233666728 - PsychologyДокумент10 страницOrder 233666728 - PsychologyLindaОценок пока нет
- Anorexia Nervosa - A Multi-Disciplinary Approach - A. Mancini (Nova, 2010) WWДокумент265 страницAnorexia Nervosa - A Multi-Disciplinary Approach - A. Mancini (Nova, 2010) WWMada AndreiОценок пока нет
- Soal Olimpiade Bahasa Inggris Guru SMAДокумент13 страницSoal Olimpiade Bahasa Inggris Guru SMACANDRA SUGI ARISTYA DEWIОценок пока нет