Вам также может понравиться
- Fever Headache Dizziness Seizure Nausea Vomiting: - X Cough DOB Constipation Diarrhea - X Abd. Pain: Location: QualityДокумент2 страницыFever Headache Dizziness Seizure Nausea Vomiting: - X Cough DOB Constipation Diarrhea - X Abd. Pain: Location: QualityJohnVincentPagadduОценок пока нет
- Systemic Response To InjuryДокумент15 страницSystemic Response To InjuryJohnVincentPagaddu100% (1)
- Critical Appraisal by John Vincent Pagaddu, M.D.Документ91 страницаCritical Appraisal by John Vincent Pagaddu, M.D.JohnVincentPagadduОценок пока нет
- Local Mechanisms Affect MAPДокумент1 страницаLocal Mechanisms Affect MAPJohnVincentPagadduОценок пока нет
- The BronchiДокумент64 страницыThe BronchiJohnVincentPagadduОценок пока нет
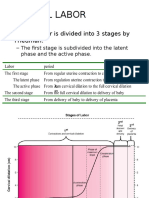
- Normal Labor: - Normal Labor Is Divided Into 3 Stages by FriedmanДокумент13 страницNormal Labor: - Normal Labor Is Divided Into 3 Stages by FriedmanJohnVincentPagadduОценок пока нет
- Self-Reliance and ProcurementДокумент16 страницSelf-Reliance and ProcurementJohnVincentPagadduОценок пока нет
- Etiology: Pneumoniae. Nontypeable Haemophilus Influenzae and Moraxella Catarrhalis May Be Significant Pathogens inДокумент4 страницыEtiology: Pneumoniae. Nontypeable Haemophilus Influenzae and Moraxella Catarrhalis May Be Significant Pathogens inJohnVincentPagadduОценок пока нет
- Bio StatisticsДокумент16 страницBio StatisticsJohnVincentPagadduОценок пока нет
- Mollusc I Pox VirusДокумент2 страницыMollusc I Pox VirusJohnVincentPagadduОценок пока нет
- Sanctity and ScarcityДокумент33 страницыSanctity and ScarcityJohnVincentPagaddu100% (1)
- HealthДокумент5 страницHealthJohnVincentPagadduОценок пока нет
- Derma Sample Exam For Practicals (Skin and Lesions)Документ42 страницыDerma Sample Exam For Practicals (Skin and Lesions)JohnVincentPagaddu100% (1)
- Surgery Ortho TraumaДокумент8 страницSurgery Ortho TraumaJohnVincentPagadduОценок пока нет
- Types of Mixtures LabДокумент2 страницыTypes of Mixtures LabJohnVincentPagadduОценок пока нет
- Population Mortality: Reported By: Group Four TFEG1 Biology 160 Lab AY 2010-2011 2 SemesterДокумент57 страницPopulation Mortality: Reported By: Group Four TFEG1 Biology 160 Lab AY 2010-2011 2 SemesterJohnVincentPagadduОценок пока нет
- Pediaortho Hand OutДокумент119 страницPediaortho Hand OutJohnVincentPagadduОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Atisara Krimi - 2018 BAMS DetailДокумент12 страницAtisara Krimi - 2018 BAMS DetailmasdfgОценок пока нет
- 2) Incaaam PP ThreadliftДокумент47 страниц2) Incaaam PP ThreadliftFitri Fratiwi100% (4)
- Orofacial CleftsДокумент19 страницOrofacial CleftsTj AngelaОценок пока нет
- An Overview of Methods Used For Estimation of Time Since Death PDFДокумент12 страницAn Overview of Methods Used For Estimation of Time Since Death PDFFajar SodiqiОценок пока нет
- Antibiotics, Misuse and ConsequencesДокумент67 страницAntibiotics, Misuse and Consequencestummalapalli venkateswara raoОценок пока нет
- GERD (Gastroesophageal Reflux Disease)Документ112 страницGERD (Gastroesophageal Reflux Disease)Mharj Alfelor Cecilio100% (7)
- ElectrocardiogramДокумент17 страницElectrocardiogramvinnu kalyanОценок пока нет
- Verbalizing Importance of Adequate Nutrition Feeds Self UnassistedДокумент2 страницыVerbalizing Importance of Adequate Nutrition Feeds Self UnassistedMasruri EfendyОценок пока нет
- SECOND Semester, AY 2022-2023: Mission VisionДокумент34 страницыSECOND Semester, AY 2022-2023: Mission Visionjeyyy BonesssОценок пока нет
- 302 PpJ. Grayson, Freedom From Obsessive Compulsive Disorder A Personalized Recovery Program For LivingДокумент2 страницы302 PpJ. Grayson, Freedom From Obsessive Compulsive Disorder A Personalized Recovery Program For LivingMohammad Shoyyad L IkhsanОценок пока нет
- Neurodegenerative DiseasesДокумент2 страницыNeurodegenerative DiseasesBerniceTanОценок пока нет
- MSDS Jun-Air SJ-27FДокумент8 страницMSDS Jun-Air SJ-27FJuan Eduardo LoayzaОценок пока нет
- Natal PlanetsДокумент290 страницNatal PlanetsAnonymous PErKNy9100% (1)
- Basic First Aid TrainingДокумент32 страницыBasic First Aid Trainingtukaram patilОценок пока нет
- Occupational Health in Indonesia: Astrid Sulistomo Dep. of Community Medicine FmuiДокумент99 страницOccupational Health in Indonesia: Astrid Sulistomo Dep. of Community Medicine FmuiDea MaharaniОценок пока нет
- Papadopoulos15 5Документ28 страницPapadopoulos15 5Ellizabeth LilantiОценок пока нет
- Vijayalakshmi MenopauseДокумент7 страницVijayalakshmi MenopauseakankshaОценок пока нет
- Spiritual Wrestling PDFДокумент542 страницыSpiritual Wrestling PDFJames CuasmayanОценок пока нет
- Suppositories Phardose LectureДокумент41 страницаSuppositories Phardose LecturePeter Paul RecaboОценок пока нет
- MenopauseДокумент21 страницаMenopauseDr K AmbareeshaОценок пока нет
- ACLS Full Lesson Plans PDFДокумент60 страницACLS Full Lesson Plans PDFVictoriano Mendez100% (1)
- Immediate Dental Implant 1Документ13 страницImmediate Dental Implant 1alkhalijia dentalОценок пока нет
- Complete DentureДокумент57 страницComplete Denturedr_ahmad_zuhdi100% (3)
- Gwich'in EthnobotanyДокумент72 страницыGwich'in EthnobotanyNatalia Alexandra Bernal QuinteroОценок пока нет
- Clinical Findings and Management of PertussisДокумент10 страницClinical Findings and Management of PertussisAGUS DE COLSAОценок пока нет
- Grand Case Pres FDARДокумент11 страницGrand Case Pres FDARMika SaldañaОценок пока нет
- Patient'S Case Performa FileДокумент13 страницPatient'S Case Performa Filevipul tandonОценок пока нет
- Esmee Sabina 19-5372 PDFДокумент3 страницыEsmee Sabina 19-5372 PDFEsme SabinaОценок пока нет
- Essene FastingДокумент48 страницEssene FastingEnoch Gandhislilbrother Abraham90% (10)
- Glove Utilization in The Prevention of Cross Transmission - A Systematic Review 2015Документ12 страницGlove Utilization in The Prevention of Cross Transmission - A Systematic Review 2015CTОценок пока нет