Вам также может понравиться
- Security Bank Personal Loan App FormДокумент2 страницыSecurity Bank Personal Loan App FormDemp Almiranez75% (4)
- First Aid Test: 367 West Robles Ave Santa Rosa, CA 95407 707-206-9988Документ15 страницFirst Aid Test: 367 West Robles Ave Santa Rosa, CA 95407 707-206-9988leesweeyaoОценок пока нет
- 2011 ACLS PretestДокумент19 страниц2011 ACLS PretestAndrew HalimОценок пока нет
- Acls CPR and Pals - Clinical Pocket GuideДокумент230 страницAcls CPR and Pals - Clinical Pocket Guideapi-275075644100% (1)
- Matrix Safety & Loss Control Overview)Документ10 страницMatrix Safety & Loss Control Overview)Rahul_Gohil_1376Оценок пока нет
- Hse Plan Asl PDFДокумент87 страницHse Plan Asl PDFBudi Prasetyo100% (1)
- Communicable Disease ChartДокумент4 страницыCommunicable Disease ChartSanjeev Kumar0% (1)
- Critical Care Calculations Study GuideДокумент6 страницCritical Care Calculations Study GuideAja Blue100% (2)
- Communicable Diseases HandoutsДокумент15 страницCommunicable Diseases HandoutsLloyd LozanoОценок пока нет
- ChickenpoxДокумент7 страницChickenpoxJennevy Buque100% (1)
- 1st Examination of Pe 12Документ4 страницы1st Examination of Pe 12Ian Santiago ParagguaОценок пока нет
- 04 - Typhoid FeverДокумент35 страниц04 - Typhoid Feversoheil100% (1)
- Principles of KinesioTaping 2014Документ29 страницPrinciples of KinesioTaping 2014Wijaya Krisna I NyomanОценок пока нет
- CHAPTER TWO Communicable DssДокумент36 страницCHAPTER TWO Communicable DssAyro Business CenterОценок пока нет
- Prenatal Factors Influencing Growth and Development of FetusДокумент15 страницPrenatal Factors Influencing Growth and Development of FetusSrd Rch100% (1)
- Typhoid FeverДокумент3 страницыTyphoid Feverdejay100Оценок пока нет
- Medical Handbook For SeafarersДокумент213 страницMedical Handbook For SeafarersmuscalualinaОценок пока нет
- Standards and Legal Aspects of IVTДокумент42 страницыStandards and Legal Aspects of IVTDemp AlmiranezОценок пока нет
- Communicable Disease ChartДокумент1 страницаCommunicable Disease ChartArlan AbraganОценок пока нет
- Table of Communicable Diseases: Disease Signs & Symptoms Incubation Prevention Chicken PoxДокумент10 страницTable of Communicable Diseases: Disease Signs & Symptoms Incubation Prevention Chicken PoxKristel_Ramall_6985Оценок пока нет
- Communicable Disease Chart Rev 3 06Документ3 страницыCommunicable Disease Chart Rev 3 06Margarrette RicoteОценок пока нет
- Feco-Orally Transmitted Diseases: (Diseases Transmitted by Contaminated Water, Food, and Others)Документ133 страницыFeco-Orally Transmitted Diseases: (Diseases Transmitted by Contaminated Water, Food, and Others)TekletsadikОценок пока нет
- CDNДокумент2 страницыCDNJohn Paulo MoralesОценок пока нет
- Communicable DiseasesДокумент10 страницCommunicable Diseaseslorenz.shinichi27Оценок пока нет
- CommunicableДокумент17 страницCommunicableJennifer Alojado TunaОценок пока нет
- Bacillary DysenteryДокумент8 страницBacillary DysenteryRijane Tabonoc OmlangОценок пока нет
- Locally Endemic DiseasesДокумент23 страницыLocally Endemic DiseasesERMIAS, ZENDY I.Оценок пока нет
- Chickenpox 160531062051 PDFДокумент16 страницChickenpox 160531062051 PDFJu Lie AnnОценок пока нет
- Synonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsДокумент13 страницSynonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsYnah DominiqueОценок пока нет
- Viral MeningitisДокумент20 страницViral MeningitisFlorence ILoyd R. TorresОценок пока нет
- Symptoms, Complications and Prevention of Typhoid FeverДокумент3 страницыSymptoms, Complications and Prevention of Typhoid Feverhasandsome100% (1)
- Health Advisory For VolunteersДокумент4 страницыHealth Advisory For VolunteersHerbert Q. CarpioОценок пока нет
- Viral InfectionsДокумент34 страницыViral InfectionsAlaa MadmoujОценок пока нет
- Name: Carlo M. Yao Bachelor of Science in NursingДокумент33 страницыName: Carlo M. Yao Bachelor of Science in Nursingcarlo24_briggsОценок пока нет
- Disa Rashe PDFДокумент2 страницыDisa Rashe PDFAlbanDedaОценок пока нет
- NCM109 - Reviewer-Lp-1-To-Lp-4Документ54 страницыNCM109 - Reviewer-Lp-1-To-Lp-4princessОценок пока нет
- Common Illnesses and Diseases of School-Aged ChildrenДокумент2 страницыCommon Illnesses and Diseases of School-Aged ChildrenKnucasior BichОценок пока нет
- Childhood Diseaases 21Документ18 страницChildhood Diseaases 21CHONAОценок пока нет
- Common Tropical DiseasesДокумент19 страницCommon Tropical DiseasesMarko TomicОценок пока нет
- A. Infectious ProcessДокумент22 страницыA. Infectious ProcessKyla Malapit GarvidaОценок пока нет
- Tuberculosis 1. Background of The Problem Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With VaricellaДокумент6 страницTuberculosis 1. Background of The Problem Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With VaricellaFkrygeustobat Tikamarimunteupercaya TanyakeunkajalminaОценок пока нет
- ChickenpoxДокумент2 страницыChickenpoxNorhana LangiОценок пока нет
- Chicken Pox HandoutsДокумент4 страницыChicken Pox Handoutsmaglangitjoannamarie1920Оценок пока нет
- Systemic Infections From GiДокумент10 страницSystemic Infections From GiJake MillerОценок пока нет
- DiseasesДокумент3 страницыDiseasesBarani KingОценок пока нет
- Dengue Fever Health TeachingДокумент9 страницDengue Fever Health TeachingChris Tine CaccamОценок пока нет
- GERMAN MEASLES and HEPATITISДокумент51 страницаGERMAN MEASLES and HEPATITISatienza02Оценок пока нет
- Emerging Disease Surveillance and ResponseДокумент4 страницыEmerging Disease Surveillance and ResponseNurusshiami KhairatiОценок пока нет
- Wa0008.Документ19 страницWa0008.Immelda Stella Medessoh DohoОценок пока нет
- Communicable Disease ChartДокумент2 страницыCommunicable Disease ChartkauragiousОценок пока нет
- Communicable DiseasesДокумент25 страницCommunicable DiseasesAbhishek DhawanОценок пока нет
- 04 - Typhoid FeverДокумент31 страница04 - Typhoid FeverGloria MachariaОценок пока нет
- Case Study of Most Common Communicable DiseasesДокумент13 страницCase Study of Most Common Communicable DiseasesnesjynОценок пока нет
- Leptospirosis: Presented By: Alexandra G de Leon Presented To: Dr. Dario V SumandeДокумент15 страницLeptospirosis: Presented By: Alexandra G de Leon Presented To: Dr. Dario V SumandealexОценок пока нет
- CD - 5th H1N1Документ40 страницCD - 5th H1N1Jannatul Adnin JinanОценок пока нет
- Lerelyn Case Reading4Документ53 страницыLerelyn Case Reading4Ma Lerelyn DatinguinooОценок пока нет
- 5.focus On Typhoid Fever PDFДокумент2 страницы5.focus On Typhoid Fever PDFBayu Surya DanaОценок пока нет
- Staph Is Short For StaphylococcusДокумент12 страницStaph Is Short For Staphylococcusdel rosarioОценок пока нет
- Dengue 1Документ6 страницDengue 1Johannah Ruth BacolodОценок пока нет
- Faeco-Oral DiseasesДокумент46 страницFaeco-Oral DiseasesNatukunda DianahОценок пока нет
- Poliomyelitis: Yahya HusseinДокумент28 страницPoliomyelitis: Yahya HusseinyahyaОценок пока нет
- Typhoid FeverДокумент12 страницTyphoid Feverlaura122334100% (1)
- Chickenpox What Is Chickenpox?Документ19 страницChickenpox What Is Chickenpox?s.khan9211rediffmail.comОценок пока нет
- Botulism: Physical ExamДокумент13 страницBotulism: Physical ExamAlexandria P. OrcajadaОценок пока нет
- Dengue Hemorrhagic Fever Nursing Considerations and Nursing Care ManagementДокумент5 страницDengue Hemorrhagic Fever Nursing Considerations and Nursing Care Managementjanns tumanengОценок пока нет
- Acute Febrile IllnessesДокумент54 страницыAcute Febrile IllnessesfraolОценок пока нет
- ChickenpoxДокумент24 страницыChickenpoxPRATIK SHRESTHAОценок пока нет
- In House COMMUNICABLE DISEASES HANDOUTДокумент10 страницIn House COMMUNICABLE DISEASES HANDOUTniczdelosreyes8Оценок пока нет
- DengueДокумент4 страницыDengueAdrian Jake LiuОценок пока нет
- Infectious Diseases: by Fares, Aya, Abdullah, Ryan and AbdulazizДокумент51 страницаInfectious Diseases: by Fares, Aya, Abdullah, Ryan and AbdulazizFares ben chaabeneОценок пока нет
- Bibliography: NCERT - TextbookДокумент10 страницBibliography: NCERT - TextbookjothiОценок пока нет
- Anatomy and Physiology of The Circulatory & Vascular SystemДокумент30 страницAnatomy and Physiology of The Circulatory & Vascular SystemDemp AlmiranezОценок пока нет
- FPFFДокумент5 страницFPFFDemp AlmiranezОценок пока нет
- Thou Hast SaidДокумент8 страницThou Hast SaidDemp AlmiranezОценок пока нет
- But God Hast Said Final 1Документ5 страницBut God Hast Said Final 1Demp AlmiranezОценок пока нет
- But God Hast Said FinalДокумент5 страницBut God Hast Said FinalDemp AlmiranezОценок пока нет
- Nurse and Midwifery - Blueprint and Reference (Dec2016) PDFДокумент2 страницыNurse and Midwifery - Blueprint and Reference (Dec2016) PDFDemp AlmiranezОценок пока нет
- Kortos Cream ENGДокумент5 страницKortos Cream ENGDemp AlmiranezОценок пока нет
- TRTRX (FTR) Tittrttffi (: Application LeaveДокумент1 страницаTRTRX (FTR) Tittrttffi (: Application LeaveDemp AlmiranezОценок пока нет
- Kortos Cream ENGДокумент5 страницKortos Cream ENGDemp AlmiranezОценок пока нет
- Read MeДокумент1 страницаRead MeChristian BagaresОценок пока нет
- NOD32 Activation KeysДокумент1 страницаNOD32 Activation KeysDemp AlmiranezОценок пока нет
- List of Assessment FeesДокумент6 страницList of Assessment FeesBenjo FransiscoОценок пока нет
- Fees EngДокумент1 страницаFees EngDemp AlmiranezОценок пока нет
- WIDESEA Company ProfileДокумент30 страницWIDESEA Company ProfileDemp AlmiranezОценок пока нет
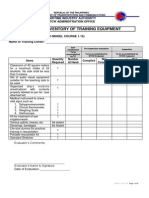
- Form 2B: Inventory of Training Equipment: Maritime Industry Authority STCW Administration OfficeДокумент9 страницForm 2B: Inventory of Training Equipment: Maritime Industry Authority STCW Administration OfficeDemp AlmiranezОценок пока нет
- Prompt ListДокумент1 страницаPrompt ListPaul ReascosОценок пока нет
- Johari WindowДокумент28 страницJohari WindowRajeev ChawlaОценок пока нет
- God of The Sky (Zoos)Документ9 страницGod of The Sky (Zoos)Demp AlmiranezОценок пока нет
- MECAДокумент2 страницыMECADemp AlmiranezОценок пока нет
- MECAДокумент2 страницыMECADemp AlmiranezОценок пока нет
- High Triglycerides: Why No Alcohol?: Prevents The Burning of FatДокумент3 страницыHigh Triglycerides: Why No Alcohol?: Prevents The Burning of FatDemp AlmiranezОценок пока нет
- Christian Daniel T. Almirañez: ObjectiveДокумент2 страницыChristian Daniel T. Almirañez: ObjectiveDemp AlmiranezОценок пока нет
- Show Me Strong Recovery - Phase 1 GuidanceДокумент8 страницShow Me Strong Recovery - Phase 1 GuidanceKevinSeanHeldОценок пока нет
- Hajj Health Management in IndonesiaДокумент2 страницыHajj Health Management in IndonesiaTeguh YuwonoОценок пока нет
- English Iv - Worksheet 1Документ2 страницыEnglish Iv - Worksheet 1Nerie BoОценок пока нет
- Quality of LifeДокумент18 страницQuality of LifeAnaghesh MuruliОценок пока нет
- Artikel Latihan Analisis HubunganДокумент11 страницArtikel Latihan Analisis HubunganRichal Grace Zefanya UlyОценок пока нет
- PSA Blueprint June2016Документ21 страницаPSA Blueprint June2016Byron Lu MorrellОценок пока нет
- Lawlor Et Al. (2017) Service User Satisfaction With CBTPДокумент19 страницLawlor Et Al. (2017) Service User Satisfaction With CBTPnuriasegarramarОценок пока нет
- NCPДокумент5 страницNCPMark John Dela CruzОценок пока нет
- Argumentative Essay: Is Meat Murder?Документ2 страницыArgumentative Essay: Is Meat Murder?Petra Gabriella PatakiОценок пока нет
- HPATHI InstrumentДокумент2 страницыHPATHI InstrumentMonika BuczmaОценок пока нет
- Health Immunization MMR FormДокумент2 страницыHealth Immunization MMR FormHenrique Delfino Almeida AlvesОценок пока нет
- SocialProgress Index 2014 ExecSummary DeloitteДокумент16 страницSocialProgress Index 2014 ExecSummary DeloitteIvan OviedoОценок пока нет
- Researches On ChallengesДокумент188 страницResearches On ChallengesMike RollideОценок пока нет
- Edinburgh Postnatal Depression Scale1 HaristaДокумент4 страницыEdinburgh Postnatal Depression Scale1 HaristaHar RealОценок пока нет
- Rice Is NiceДокумент3 страницыRice Is Niceammayi100Оценок пока нет
- Revealing What Is Distinct by Recognising What Is Common: Distinguishing Between Complex PTSD and Borderline Personality Disorder Symptoms Using Bifactor Modelling 2020Документ10 страницRevealing What Is Distinct by Recognising What Is Common: Distinguishing Between Complex PTSD and Borderline Personality Disorder Symptoms Using Bifactor Modelling 2020Nicolás MaturanaОценок пока нет
- Star T30 1720 3710321125 enДокумент200 страницStar T30 1720 3710321125 enJ WОценок пока нет
- Gianna Graziani Cover LetterДокумент1 страницаGianna Graziani Cover Letterapi-733890262Оценок пока нет
- Objectives: Your QuestiensДокумент8 страницObjectives: Your Questiensjoel zapanaОценок пока нет
- IДокумент14 страницIjasdeepkaurnagra100% (1)
- Company Information JohnsonДокумент18 страницCompany Information JohnsonPriya JeevaОценок пока нет
- Dental AbscessДокумент14 страницDental Abscessvinnu kalyanОценок пока нет
- SSR ADVISORY - Use of Sansure Storage Reagent For LGU-DRUДокумент3 страницыSSR ADVISORY - Use of Sansure Storage Reagent For LGU-DRUFret Ramirez Coronia RNОценок пока нет
- Antibiotik Dan Antiseptik Sal KemihДокумент23 страницыAntibiotik Dan Antiseptik Sal KemihruuweelscribdОценок пока нет
- Acute Pain Nursing Care PlanДокумент3 страницыAcute Pain Nursing Care PlanSiafei RabeОценок пока нет