Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Drug Name Indication: Action: Mechanism of Action Classificatio N Adverse Effects Contraindications: Nursing ConsiderationsДокумент2 страницыDrug Name Indication: Action: Mechanism of Action Classificatio N Adverse Effects Contraindications: Nursing ConsiderationsEsmareldah Henry SirueОценок пока нет
- Psychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsДокумент18 страницPsychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDrima EdiОценок пока нет
- Benadryl Allergy Children's 1mg - ML Oral Solution - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Документ8 страницBenadryl Allergy Children's 1mg - ML Oral Solution - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)WenChin FooОценок пока нет
- Resume SsureshДокумент20 страницResume SsureshAdinarayana ReddyОценок пока нет
- Procedure of General AnaesthesiaДокумент4 страницыProcedure of General AnaesthesiaNuridayu Sedek100% (1)
- RGUHS - BPT - 2019 - 2 - Apr - 2710 Pharmacology (Rs 3 and Rs 4)Документ1 страницаRGUHS - BPT - 2019 - 2 - Apr - 2710 Pharmacology (Rs 3 and Rs 4)Nuhman Abdu RahmanОценок пока нет
- Drug ResearchДокумент33 страницыDrug ResearchJakobus Benny SalimОценок пока нет
- Immuno Oncology Therapies White Paper PPDДокумент12 страницImmuno Oncology Therapies White Paper PPDkevalОценок пока нет
- CH 19-Noninvasive VentilationДокумент65 страницCH 19-Noninvasive VentilationGhaida AlshehriОценок пока нет
- Paediatric Resuscitation, Stabilisation Retrieval and TransferДокумент12 страницPaediatric Resuscitation, Stabilisation Retrieval and TransferSri HariОценок пока нет
- Prioritization of Mabs During Resource Shortages 20211229Документ3 страницыPrioritization of Mabs During Resource Shortages 20211229News10NBCОценок пока нет
- Medication Card Case.2Документ6 страницMedication Card Case.2Jemina Rafanan RacadioОценок пока нет
- Annotated BibliographyДокумент5 страницAnnotated Bibliographyapi-273602090Оценок пока нет
- Talak KejangДокумент52 страницыTalak KejangRiga Medina IIОценок пока нет
- Compounding in Community SettingДокумент19 страницCompounding in Community Settingkhangsiean89100% (1)
- 2nd LectureДокумент22 страницы2nd Lecturenwekar groupОценок пока нет
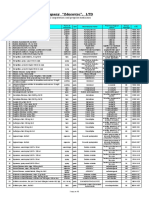
- Pharmaceutical Company "Zdorovye", LTD: Price-List (USD) 03.09.2019Документ10 страницPharmaceutical Company "Zdorovye", LTD: Price-List (USD) 03.09.2019Laura Del valleОценок пока нет
- PHARMACOLOGYДокумент19 страницPHARMACOLOGYIligan, JamaicahОценок пока нет
- Resuscitation Trolley Checklist: RrcsuДокумент7 страницResuscitation Trolley Checklist: RrcsuPatrick SimembaОценок пока нет
- Adr and ManagementДокумент48 страницAdr and ManagementDhanush G V DhanushОценок пока нет
- Special Articles: Awake Intubation Intubation After Induction of General AnesthesiaДокумент1 страницаSpecial Articles: Awake Intubation Intubation After Induction of General AnesthesiaOKE channelОценок пока нет
- Pemakaian April 2022Документ9 страницPemakaian April 2022nurulОценок пока нет
- Tatalaksana ACS HUT Harkit 2015 - 1 PDFДокумент35 страницTatalaksana ACS HUT Harkit 2015 - 1 PDFKevin EdroОценок пока нет
- DextromethorphanДокумент6 страницDextromethorphanAbdelrhman AboodaОценок пока нет
- Fluid Therapy in Cardiac Surgery PatientsДокумент37 страницFluid Therapy in Cardiac Surgery PatientsaymxОценок пока нет
- Critical Appraisal HARM STUDY - Prof AtiДокумент23 страницыCritical Appraisal HARM STUDY - Prof AtiM Nadim MulachelaОценок пока нет
- Actualización en El Manejo Médico Del Cáncer de Cérvix Recurrente - Bradley MonkДокумент35 страницActualización en El Manejo Médico Del Cáncer de Cérvix Recurrente - Bradley Monkinfo7615Оценок пока нет
- ParacetamolДокумент3 страницыParacetamolKrla Jaimee BulaОценок пока нет
- Anesthesia For The Obese PatientДокумент24 страницыAnesthesia For The Obese PatientCharlieBrown_QBОценок пока нет
- Drug Development ProcessДокумент16 страницDrug Development ProcessNachiket PatelОценок пока нет