Вам также может понравиться
- 1.emollients Prescribing Guideline Sept 2013Документ4 страницы1.emollients Prescribing Guideline Sept 2013kyle31Оценок пока нет
- Necessary Elements of A Dermatologic History and Physical Evaluation PDFДокумент9 страницNecessary Elements of A Dermatologic History and Physical Evaluation PDFkyle31Оценок пока нет
- Taking A Dermatological History - Dermatology - FastbleepДокумент5 страницTaking A Dermatological History - Dermatology - Fastbleepkyle31Оценок пока нет
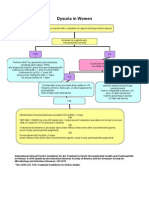
- Women With Dysuria AlgorhtmДокумент1 страницаWomen With Dysuria Algorhtmkyle31Оценок пока нет
- AntihypertensiveДокумент1 страницаAntihypertensivekyle31Оценок пока нет
- Marsupialization of A Bartholin's Cyst or AbscessДокумент2 страницыMarsupialization of A Bartholin's Cyst or Abscesskyle31Оценок пока нет
- A Brief Review: The Epidemiology of Acquired Melanocytic NeviДокумент9 страницA Brief Review: The Epidemiology of Acquired Melanocytic Nevikyle31Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- 1.3.1 The Autopsy-1Документ4 страницы1.3.1 The Autopsy-1Alyssa robertsОценок пока нет
- Introduction and Analytical Report PDFДокумент111 страницIntroduction and Analytical Report PDFJoão Pedro GarciaОценок пока нет
- Training 11 Add 3 enДокумент44 страницыTraining 11 Add 3 enBela CruzОценок пока нет
- Biodata Format FinalДокумент5 страницBiodata Format FinalCharles Saurus PacomaОценок пока нет
- June02.2016 Bbill Calls For Monitoring of Absences To Curb AbsenteeismДокумент2 страницыJune02.2016 Bbill Calls For Monitoring of Absences To Curb Absenteeismpribhor2Оценок пока нет
- Operation Management ReportДокумент12 страницOperation Management ReportMuntaha JunaidОценок пока нет
- Fun Games - 1 Min Game 01Документ9 страницFun Games - 1 Min Game 01Purvi ShahОценок пока нет
- Rules Related Statutes All CodesДокумент150 страницRules Related Statutes All CodesRod SatreОценок пока нет
- ErpДокумент31 страницаErpNurul Badriah Anwar AliОценок пока нет
- Gefico Maritime SectorДокумент28 страницGefico Maritime SectorAugustine Dharmaraj100% (1)
- Dental Trauma - An Overview of Its Influence On The Management of Orthodontic Treatment - Part 1.Документ11 страницDental Trauma - An Overview of Its Influence On The Management of Orthodontic Treatment - Part 1.Djoka DjordjevicОценок пока нет
- QR CPG TobacoDisorderДокумент8 страницQR CPG TobacoDisorderiman14Оценок пока нет
- Pediatric Blood PressureДокумент28 страницPediatric Blood PressureGenta Syaifrin Laudza0% (1)
- Questionnaire For Stress Management in An OrganizationДокумент8 страницQuestionnaire For Stress Management in An OrganizationTapassya Giri33% (3)
- Boracay Rehabilitation: A Case StudyДокумент9 страницBoracay Rehabilitation: A Case StudyHib Atty TalaОценок пока нет
- Tinetti Assessment BalanceДокумент2 страницыTinetti Assessment Balancesathish Lakshmanan100% (1)
- A Study On Pandemic Related Challenges Faced in Rural Areas: Patel Preja ID No: 20BBA125Документ9 страницA Study On Pandemic Related Challenges Faced in Rural Areas: Patel Preja ID No: 20BBA125PREJA PATELОценок пока нет
- Gagan ResumeДокумент6 страницGagan Resumedrgaganwahi100% (2)
- Cancer Genetics-Genetic InstabilityДокумент60 страницCancer Genetics-Genetic InstabilityMadhu MithaОценок пока нет
- Analysis of Shift in Consumption of Carbonated Beverages To Healthy DrinksДокумент26 страницAnalysis of Shift in Consumption of Carbonated Beverages To Healthy DrinksAntara JasrotiaОценок пока нет
- Top 10 Regulatory Challenges in The Healthcare EnvironmentДокумент3 страницыTop 10 Regulatory Challenges in The Healthcare EnvironmentNicki BombezaОценок пока нет
- Lesson 2 Prepare Cereal and StarchДокумент25 страницLesson 2 Prepare Cereal and StarchLieybeem Vergara50% (2)
- Course Profile - HIRARC - 1 DAYДокумент4 страницыCourse Profile - HIRARC - 1 DAYRizal de silvaОценок пока нет
- Sistem Pakar Diagnosis Penyakit Pada Ayam Dengan Menggunakan Metode Dempster ShaferДокумент11 страницSistem Pakar Diagnosis Penyakit Pada Ayam Dengan Menggunakan Metode Dempster ShaferYata RinОценок пока нет
- India's #1 Nroute Daily Whey Protein Powder Online 2022Документ3 страницыIndia's #1 Nroute Daily Whey Protein Powder Online 2022NRoute ProteinОценок пока нет
- Ada 2018Документ174 страницыAda 2018CarlosChávezОценок пока нет
- Administration of PICU Child Health NursingДокумент37 страницAdministration of PICU Child Health NursingJimcy100% (3)
- Understanding Desistance From Crime Laub and SampsonДокумент70 страницUnderstanding Desistance From Crime Laub and Sampsonchrisgoss1Оценок пока нет
- Pollution of The WaterДокумент25 страницPollution of The WaterJeprox Martinez100% (1)
- Dentistry Indonesia, 20 (1), 5-8.: Daftar PustakaДокумент6 страницDentistry Indonesia, 20 (1), 5-8.: Daftar PustakaSari RahayuniОценок пока нет