Вам также может понравиться
- Phil Telegraph Vs PeopleДокумент11 страницPhil Telegraph Vs PeopleRachelle DomingoОценок пока нет
- Ollendorf Vs Abrahamson, 38 Phil. 585Документ7 страницOllendorf Vs Abrahamson, 38 Phil. 585Jane Kirsty PaulineОценок пока нет
- 20 - Del Monte vs. VelascoДокумент6 страниц20 - Del Monte vs. VelascojannahОценок пока нет
- Phil Telegraph Vs PeopleДокумент11 страницPhil Telegraph Vs PeopleRachelle DomingoОценок пока нет
- Del Castillo V RichmondДокумент5 страницDel Castillo V RichmondPatrick GallitoОценок пока нет
- Del Castillo V RichmondДокумент5 страницDel Castillo V RichmondPatrick GallitoОценок пока нет
- 17 US Vs PalacioДокумент6 страниц17 US Vs PalacioAngeline LimpiadaОценок пока нет
- 9 Tiger Construction V AbayДокумент10 страниц9 Tiger Construction V Abaybraindead_91Оценок пока нет
- 20 - Del Monte vs. VelascoДокумент6 страниц20 - Del Monte vs. VelascojannahОценок пока нет
- 4 Sapio V UndalocДокумент12 страниц4 Sapio V Undalocbraindead_91Оценок пока нет
- 8 Philippine Hoteliers V National Union of Workers in HotelsДокумент14 страниц8 Philippine Hoteliers V National Union of Workers in Hotelsbraindead_91Оценок пока нет
- RFP Lawyers GuideДокумент42 страницыRFP Lawyers Guide*Luciola*Оценок пока нет
- 7 Jethro V SOLEДокумент9 страниц7 Jethro V SOLEbraindead_91Оценок пока нет
- Leal V IACДокумент9 страницLeal V IACChaОценок пока нет
- Paflu Vs Sec of LaborДокумент6 страницPaflu Vs Sec of Laboryanex2Оценок пока нет
- Floresca Vs Philex Mining CorpДокумент33 страницыFloresca Vs Philex Mining Corpbraindead_91Оценок пока нет
- 07 Lichauco Vs Apostol GR 19628Документ11 страниц07 Lichauco Vs Apostol GR 19628Greg MarilynОценок пока нет
- People v. JabinalДокумент6 страницPeople v. JabinalJulian Paul CachoОценок пока нет
- Paflu Vs Sec of LaborДокумент6 страницPaflu Vs Sec of Laboryanex2Оценок пока нет
- Apiag Vs CanteroДокумент11 страницApiag Vs CanteroClaire Cortez CruzОценок пока нет
- 17 US Vs PalacioДокумент6 страниц17 US Vs PalacioAngeline LimpiadaОценок пока нет
- Phil Rabbit Bus Lines Vs Arciaga GR No L-29701 16mar1987Документ4 страницыPhil Rabbit Bus Lines Vs Arciaga GR No L-29701 16mar1987braindead_91Оценок пока нет
- 75 Dy Teban vs. ChingДокумент22 страницы75 Dy Teban vs. Chingbryan planaОценок пока нет
- Bernabe Vs Alejo GR No 140500 21jan2002Документ8 страницBernabe Vs Alejo GR No 140500 21jan2002braindead_91Оценок пока нет
- Endencia v. David G.R. No. L-6355-56 August 31, 1953Документ6 страницEndencia v. David G.R. No. L-6355-56 August 31, 1953jon_cpaОценок пока нет
- 2009 Arangote - v. - Spouses - Maglunob20181001 5466 l6ft93 PDFДокумент13 страниц2009 Arangote - v. - Spouses - Maglunob20181001 5466 l6ft93 PDFbraindead_91Оценок пока нет
- LASCO, Paulo M.: PRO VersionДокумент6 страницLASCO, Paulo M.: PRO Versionbraindead_91Оценок пока нет
- ALBANO, Chalum B. (SUMALBAG, Henrietta B.) : PRO VersionДокумент8 страницALBANO, Chalum B. (SUMALBAG, Henrietta B.) : PRO Versionbraindead_91Оценок пока нет
- Republic v. Intermediate Appellate Court20190502-5466-G9x1fiДокумент8 страницRepublic v. Intermediate Appellate Court20190502-5466-G9x1fiBingkatify McarimbangОценок пока нет
- Notice of Appeal SampleДокумент1 страницаNotice of Appeal SampleJose Cabrera JrОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
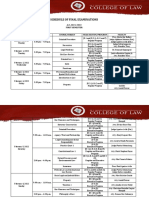
- 1st Sem 2021 22 Finals ScheduleДокумент5 страниц1st Sem 2021 22 Finals ScheduleRyan ChristianОценок пока нет
- Polonsky Vs WellsДокумент32 страницыPolonsky Vs WellsZerohedgeОценок пока нет
- Roadtec SB-2500B MANUALSpdf PDFДокумент112 страницRoadtec SB-2500B MANUALSpdf PDFChristian Rejón Sánchez100% (3)
- As365-Ec155-Sa365 2021-03-06Документ7 страницAs365-Ec155-Sa365 2021-03-06chiri003Оценок пока нет
- Gustavo A. de La Vega v. Alberto R. Gonzales, Attorney General of The United States, Edward McElroy New York District Director, Immigration and Naturalization Service, 436 F.3d 141, 2d Cir. (2006)Документ8 страницGustavo A. de La Vega v. Alberto R. Gonzales, Attorney General of The United States, Edward McElroy New York District Director, Immigration and Naturalization Service, 436 F.3d 141, 2d Cir. (2006)Scribd Government DocsОценок пока нет
- 0002773-Florida Laws and RulesДокумент151 страница0002773-Florida Laws and RulesPDHLibraryОценок пока нет
- EDI Restructuring, or Putting The REDs To BedДокумент2 страницыEDI Restructuring, or Putting The REDs To BedChris YellandОценок пока нет
- Tertangkap Tangan Perkara Tindak Pidana Korupsi Dalam Perspektif Nilai Kepastian HukumДокумент20 страницTertangkap Tangan Perkara Tindak Pidana Korupsi Dalam Perspektif Nilai Kepastian HukumHendij O. TololiuОценок пока нет
- Chapter 22Документ5 страницChapter 22api-235651608Оценок пока нет
- General Exceptions To IPCДокумент14 страницGeneral Exceptions To IPCNidhi SinghОценок пока нет
- Manalo vs. Court of AppealsДокумент4 страницыManalo vs. Court of AppealsaudreyracelaОценок пока нет
- The Economic Loss DoctrineДокумент9 страницThe Economic Loss DoctrineK CorОценок пока нет
- Complainant,: Complaint-Affidavit THE UNDERSIGNED COMPLAINANT Respectfully AllegesДокумент5 страницComplainant,: Complaint-Affidavit THE UNDERSIGNED COMPLAINANT Respectfully AllegesBeta Sigma Lambda Marawi ChapterОценок пока нет
- Sample Affidavit To The Company For Time Gap in JoiningДокумент2 страницыSample Affidavit To The Company For Time Gap in Joiningwww.aletterformat.com100% (1)
- Insulin Action - Hagens Berman Application For Interim Leadership 2017-05Документ27 страницInsulin Action - Hagens Berman Application For Interim Leadership 2017-05The Type 1 Diabetes Defense FoundationОценок пока нет
- Omnibus Certification of Authenticity and Veracity of All Documents SubmittedДокумент1 страницаOmnibus Certification of Authenticity and Veracity of All Documents SubmittedRaulen Jereos91% (45)
- 2013 Nissan Gallery Ortigas v. FelipeДокумент6 страниц2013 Nissan Gallery Ortigas v. FelipeGermaine CarreonОценок пока нет
- (1957) East Africa Law ReportsДокумент1 581 страница(1957) East Africa Law ReportsRobert Walusimbi82% (11)
- Ponce de Leon V RFCДокумент103 страницыPonce de Leon V RFCAiyla AnonasОценок пока нет
- Labor 2 Reviewer-YapKДокумент12 страницLabor 2 Reviewer-YapKKrystoffer YapОценок пока нет
- Pnb-Republic Bank V. NLRC GR No. 117460 January 6, 1997Документ3 страницыPnb-Republic Bank V. NLRC GR No. 117460 January 6, 1997compiler123Оценок пока нет
- DM - 2023 Celebration of NCMДокумент2 страницыDM - 2023 Celebration of NCMJoanna Marie MenorОценок пока нет
- Buy Back of Shares: - Secretarial PracticeДокумент6 страницBuy Back of Shares: - Secretarial PracticecoolsikhОценок пока нет
- LC DigestДокумент34 страницыLC DigestJuvylynPiojoОценок пока нет
- Contract ActДокумент32 страницыContract ActMonika KauraОценок пока нет
- PP V Teo Eng Chan & Ors Case ReviewДокумент4 страницыPP V Teo Eng Chan & Ors Case ReviewLingXiiaoОценок пока нет
- Business Law Chapter02Документ27 страницBusiness Law Chapter02jmartinez35071% (7)
- R S CPC: Epresentative Uits UnderДокумент18 страницR S CPC: Epresentative Uits UnderektaОценок пока нет
- Landmark Cases On Arbitration in IndiaДокумент3 страницыLandmark Cases On Arbitration in IndiaabhaykachchhawahОценок пока нет
- Uy Tong vs. Silva, 132 SCRA 448Документ2 страницыUy Tong vs. Silva, 132 SCRA 448Joshua AmistosoОценок пока нет