Вам также может понравиться
- 2018 STEM Institute BrochureДокумент2 страницы2018 STEM Institute BrochureStem InstОценок пока нет
- 2018 STEM Institute Brochure Vs 1Документ3 страницы2018 STEM Institute Brochure Vs 1Stem InstОценок пока нет
- 2017 STEM Institute BrochureДокумент3 страницы2017 STEM Institute BrochureStem InstОценок пока нет
- 2017 STEM Institute BrochureДокумент3 страницы2017 STEM Institute BrochureStem InstОценок пока нет
- 2016 STEM Institute BrochureДокумент2 страницы2016 STEM Institute BrochureStem InstОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Betterment Demographics ReportДокумент6 страницBetterment Demographics ReportConnor LeeОценок пока нет
- CDS6 and CDS7 Billing CodesДокумент9 страницCDS6 and CDS7 Billing CodesMatthew BellusciОценок пока нет
- The History and Experience of Latinos/Hispanics in The United States Ana Maria Pineda, R.S.MДокумент16 страницThe History and Experience of Latinos/Hispanics in The United States Ana Maria Pineda, R.S.MbauemmvssОценок пока нет
- Ethnic Minorities in The UsaДокумент5 страницEthnic Minorities in The UsaTīzīrī ĔşpiОценок пока нет
- Teaching of Psychology: Sniffing Out Efficacy: Sniffy Lite, A Virtual Animal LabДокумент4 страницыTeaching of Psychology: Sniffing Out Efficacy: Sniffy Lite, A Virtual Animal LabPilu DrubeОценок пока нет
- Macroeconomics Questions 2Документ59 страницMacroeconomics Questions 2Hoàng Thanh Tùng (FE FPTU HN)Оценок пока нет
- UH Manoa Honolulu Houseless ReportДокумент51 страницаUH Manoa Honolulu Houseless ReportHawaii Public RadioОценок пока нет
- Complaint Form For Allegations of Program Discrimination by The Social Security Administration InstructionsДокумент8 страницComplaint Form For Allegations of Program Discrimination by The Social Security Administration InstructionsAfzal ImamОценок пока нет
- Marist Poll For Georgia RacesДокумент35 страницMarist Poll For Georgia RacesLindsey BasyeОценок пока нет
- A Parent-Report Instrument For Identifying One-Year-Olds Risk TEAДокумент20 страницA Parent-Report Instrument For Identifying One-Year-Olds Risk TEADani Tsu100% (1)
- Community Needs Assessment QuestionnaireДокумент12 страницCommunity Needs Assessment Questionnaireawit tiradОценок пока нет
- LRAP 2020 Report Preliminary Sum Sept. 30Документ10 страницLRAP 2020 Report Preliminary Sum Sept. 30ennylemОценок пока нет
- St. LouisДокумент20 страницSt. LouisJulianaRocjОценок пока нет
- DD2808Report of Medical ExaminationДокумент3 страницыDD2808Report of Medical Examinationk_tanjaОценок пока нет
- CRF Design Template v4.0Документ28 страницCRF Design Template v4.0Shalini ShivenОценок пока нет
- WKEC KYAD Enrollment Form 2022 2023-FillableДокумент2 страницыWKEC KYAD Enrollment Form 2022 2023-FillableNaung Ainn TawОценок пока нет
- The Nation's Report Card Mathematics 2009Документ68 страницThe Nation's Report Card Mathematics 2009GothamSchools.orgОценок пока нет
- Calapa c1 s1 DatacollectionsummaryДокумент4 страницыCalapa c1 s1 Datacollectionsummaryapi-39989174488% (8)
- Van Hoa MyДокумент60 страницVan Hoa Mythanhduom100% (1)
- Application For Waiver of Grounds of Inadmissibility: Uscis Form I-601Документ12 страницApplication For Waiver of Grounds of Inadmissibility: Uscis Form I-601Yorge Alberto PerezОценок пока нет
- Ch.1-16 Answers Combined Upload FileДокумент144 страницыCh.1-16 Answers Combined Upload Filebrandon culpepper71% (7)
- Inner Temple ApplicationДокумент25 страницInner Temple ApplicationSayedulОценок пока нет
- The Alternative Hypothesis: Re-Examining The JQДокумент53 страницыThe Alternative Hypothesis: Re-Examining The JQBlack Sheep Brouhaha100% (1)
- DD 1966Документ6 страницDD 1966gabepezОценок пока нет
- Grand Vision: Land Use Values SurveyДокумент53 страницыGrand Vision: Land Use Values SurveyGary HoweОценок пока нет
- Instructions For Completing Enrollment Application For Health BenefitsДокумент5 страницInstructions For Completing Enrollment Application For Health BenefitsDonna Mae RafolОценок пока нет
- 105 Parents Birth WorksheetДокумент9 страниц105 Parents Birth WorksheetKUTV 2NewsОценок пока нет
- Latino Group Consciousness and Political ParticipationДокумент19 страницLatino Group Consciousness and Political ParticipationMagda BoОценок пока нет
- Yahoo! News SurveyДокумент102 страницыYahoo! News SurveyJack ForbesОценок пока нет
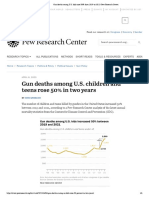
- Gun Deaths Among U.S. Kids Rose 50% From 2019 To 2021 - Pew Research CenterДокумент6 страницGun Deaths Among U.S. Kids Rose 50% From 2019 To 2021 - Pew Research CenterNguyễn Thị Tú OanhОценок пока нет